⚕️ Medical Disclosure Vitamin D deficiency is a medical condition that should be confirmed by blood test (25-hydroxyvitamin D). The symptoms described in this article overlap with many other conditions — do not self-diagnose deficiency based on symptoms alone. If you experience the symptoms described here, request a 25(OH)D blood test from your physician. Adults with kidney disease, hyperparathyroidism, sarcoidosis, or lymphoma should not supplement vitamin D without physician guidance. This article does not constitute medical advice.
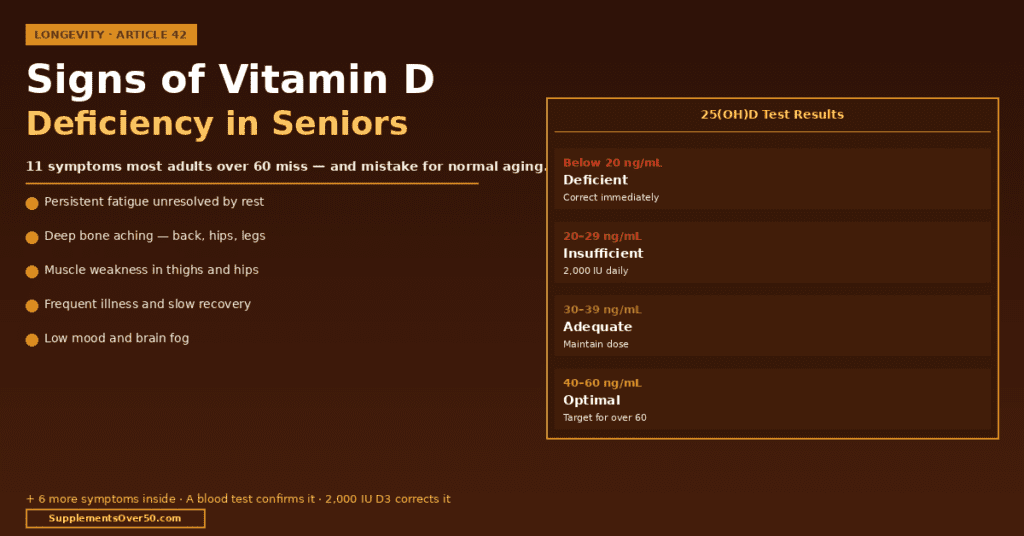
⚡ Quick Answer — Key Statistics 42% of US adults are vitamin D deficient. Among adults over 65, Signs of Vitamin D Deficiency in Seniors is quite evident, the rate rises to approximately 50–60% due to the 75% decline in skin synthesis efficiency that occurs between ages 20 and 70. The most common symptoms of deficiency — fatigue, muscle weakness, bone aches, and low mood — are frequently attributed to normal aging rather than to a correctable nutritional deficit. A simple blood test for 25-hydroxyvitamin D (25(OH)D) is the only reliable way to confirm deficiency. The threshold: below 20 ng/mL is deficient, 20–29 ng/mL is insufficient, 30–50 ng/mL is adequate, and 40–60 ng/mL is the optimal range for adults over 60 based on current evidence.
Why Vitamin D Deficiency Is So Common After 60 — And So Frequently Missed
Vitamin D deficiency has a paradox at its core: it is among the most common nutritional deficiencies in older adults and among the most frequently overlooked by both patients and physicians. The symptoms mimic normal aging so closely — fatigue, muscle weakness, aching bones, low mood, frequent illness — that millions of adults over 60 experience years of correctable deficiency while attributing every symptom to simply ‘getting older.’
Three biological changes converge after 60 to make deficiency nearly inevitable without supplementation. First, skin synthesis efficiency declines approximately 75% between ages 20 and 70 — the same amount of sun exposure that produces 1,000 IU of vitamin D in a young adult produces only 250 IU in a 70-year-old. Second, kidney function declines with age, reducing the conversion of storage vitamin D (25-hydroxyvitamin D) to the active hormone form (1,25-dihydroxyvitamin D). Third, the dietary sources of vitamin D — fatty fish, egg yolks, fortified dairy — are often reduced in seniors eating lighter, smaller meals.
The result: even seniors who spend time outdoors, eat reasonably, and take a standard multivitamin commonly test deficient. The 600–800 IU found in most multivitamins was set to prevent rickets — not to maintain the 40–60 ng/mL blood levels associated with optimal muscle function, immune response, cardiovascular health, and cognitive performance in older adults.
42% of US adults are vitamin D deficient (25(OH)D below 20 ng/mL) — rising to approximately 50–60% in adults over 65
Skin synthesis efficiency declines 75% between ages 20 and 70 — making supplementation effectively mandatory for most seniors regardless of sun exposure
Vitamin D receptors (VDRs) are present in over 30 tissues including muscle, brain, immune cells, cardiovascular tissue, and the gut — explaining why deficiency produces such a diverse symptom picture
A 2018 meta-analysis of 25 RCTs found vitamin D supplementation reduced all-cause mortality in older adults by 12% — the largest mortality reduction of any single supplement studied
Vitamin D deficiency doubles the risk of falls in adults over 65 by impairing fast-twitch muscle fibre function and balance response
Low vitamin D is associated with a 40% higher risk of depression in adults over 60 in large population studies
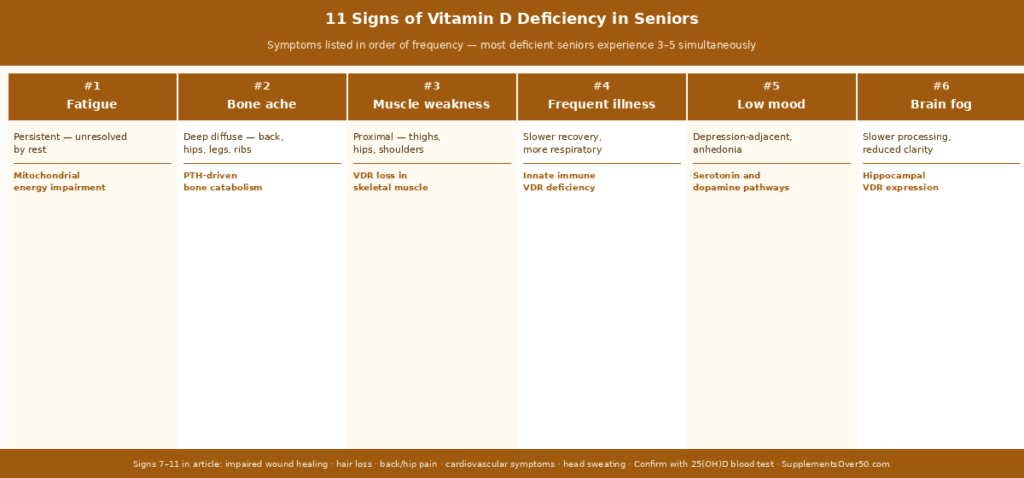
The 11 Signs of Vitamin D Deficiency in Seniors
These symptoms are listed in order of how commonly they are reported in deficient adults over 60. Most deficient seniors experience at least 3–4 of these simultaneously — the clustering pattern is itself a diagnostic signal.
Fatigue is the most frequently reported symptom of vitamin D deficiency in older adults and the one most often dismissed as normal aging. The mechanism is direct: vitamin D is required for mitochondrial function in skeletal and cardiac muscle cells — it regulates the expression of genes involved in ATP production. Without adequate vitamin D, cellular energy generation is impaired at the most fundamental level. Seniors describe this as a fatigue that is present regardless of sleep quality — a heaviness or low energy that persists through the day even after a full night’s rest.
Key distinguishing feature: vitamin D fatigue typically improves significantly within 4–8 weeks of corrective supplementation. If fatigue resolves with D3 correction, deficiency was likely the primary driver.
2. Bone Aches and Deep Bone Pain
Vitamin D deficiency impairs calcium absorption from the gut and increases parathyroid hormone (PTH) production. Elevated PTH causes the body to draw calcium from bones to maintain blood calcium levels — producing the bone thinning that leads to osteopenia and osteoporosis in the long term. In the shorter term, the metabolic changes cause a characteristic deep, diffuse aching in the bones — most commonly in the lower back, hips, legs, and ribs. This is distinct from joint pain (which is at the joints) — bone pain is in the shaft of the bone itself.
Many seniors describe this as an aching discomfort that worsens at night or with pressure on the bone. It is frequently attributed to arthritis. The distinguishing question: does the pain localise to joints (more likely arthritis) or is it diffuse and in the bone itself (more likely vitamin D deficiency or osteomalacia)?
Vitamin D receptors are expressed in skeletal muscle tissue and directly regulate fast-twitch muscle fibre development and function. Fast-twitch fibres are the fibres used for sudden movements — standing up quickly, catching a balance stumble, climbing stairs. Deficiency produces a characteristic proximal muscle weakness (affecting muscles closest to the trunk — thighs, hips, shoulders) that manifests as difficulty getting up from a chair without using arms, difficulty climbing stairs, and general lower limb weakness.
This is clinically significant because proximal muscle weakness is a primary fall risk factor in seniors. A 2011 meta-analysis found vitamin D supplementation reduced fall risk by 19% through this exact muscle spindle mechanism.
Vitamin D is one of the most important modulators of immune function in older adults. VDRs are present on virtually every immune cell type — T cells, B cells, natural killer cells, and macrophages. Vitamin D activates genes that produce antimicrobial peptides (defensins and cathelicidins) that form the first line of defence against respiratory pathogens. Deficient seniors show reduced innate immune responsiveness — taking longer to recover from infections, experiencing more frequent respiratory illnesses, and showing blunted vaccine responses in some studies.
The practical signal: if you are getting sick more often than you were 5–10 years ago, or taking noticeably longer to recover from colds and minor infections, vitamin D deficiency should be assessed alongside other immune health factors.
5. Low Mood and Depression
Vitamin D receptors are expressed in the brain regions involved in mood regulation — the prefrontal cortex, hippocampus, and cingulate cortex. Vitamin D influences serotonin synthesis and dopamine receptor function through these receptors. Large population studies consistently find low vitamin D status is associated with significantly higher rates of depression in adults over 60. A 2020 meta-analysis found vitamin D supplementation produced significant improvements in depression scores in adults with confirmed deficiency.
The clinical pattern: if low mood, pessimism, or mild anhedonia (reduced pleasure in activities) has increased noticeably over the past 1–2 years — and is not explained by major life stressors or psychiatric history — vitamin D deficiency is worth excluding with a blood test before attributing mood changes to aging.
6. Impaired Wound Healing
Vitamin D plays a role in all four phases of wound healing — haemostasis, inflammation, proliferation, and remodelling. Deficient seniors frequently notice that minor cuts, bruises, and skin injuries take longer to heal than they used to. Surgical wound healing is also impaired in deficient patients. If you are having dental work, surgery, or any procedure and have not checked your vitamin D status, pre-operative optimisation of D3 levels is worth discussing with your physician.
7. Hair Loss — Particularly Diffuse Thinning
Vitamin D stimulates hair follicle cycling and is involved in keratinocyte differentiation in the scalp. Deficiency is associated with telogen effluvium — diffuse hair thinning across the scalp rather than pattern hair loss. In older women, diffuse hair thinning is frequently attributed to menopause — and while hormonal changes contribute, vitamin D deficiency is a co-factor that is frequently overlooked and correctable. In men, vitamin D deficiency can accelerate the diffuse thinning that accompanies age-related hormonal changes.
8. Back Pain and Hip Pain
The relationship between vitamin D deficiency and back pain is well-documented. A 2015 systematic review found deficient adults have significantly higher rates of chronic low back pain. The mechanism combines the bone ache of early osteomalacia with the muscle weakness-related postural strain from reduced core and hip muscle strength. Hip pain that worsens with weight-bearing and is not clearly articular (not at the hip joint itself) should prompt vitamin D assessment alongside x-ray evaluation.
9. Cognitive Decline and Brain Fog
Vitamin D receptors in the brain regulate neuroprotective genes, amyloid clearance, and inflammatory pathways. Low vitamin D is associated in population studies with accelerated cognitive decline and higher dementia risk. The most common cognitive manifestation of deficiency is not frank memory loss but rather brain fog — reduced mental clarity, slower information processing, and difficulty concentrating that seniors often describe as ‘the mental sharpness I used to have.’ This frequently appears years before any measurable memory deficit on formal testing.
This vitamin D deficiency cognitive symptom overlaps with the symptoms that phosphatidylserine and citicoline address — suggesting that seniors with brain fog may benefit from addressing vitamin D deficiency alongside targeted brain supplement support.
Vitamin D receptors are expressed in cardiac muscle and vascular smooth muscle. Deficiency is associated with higher blood pressure, increased arterial stiffness, and higher rates of cardiovascular events in epidemiological studies. At the symptomatic level, some deficient patients report palpitations — which may be related to vitamin D’s role in cardiac calcium handling and electrolyte balance — and reduced exercise tolerance. These symptoms always warrant physician evaluation to exclude primary cardiac causes before attributing them to vitamin D deficiency.
11. Sweating of the Head
Excessive sweating of the forehead and scalp — not explained by room temperature or exertion — is a classic but under-recognised historical sign of vitamin D deficiency (historical medical texts described ‘profuse head sweating’ as a rickets symptom). While this sign is far less specific than the others listed, its presence alongside three or more of the above symptoms significantly increases the probability of deficiency. If you are sweating disproportionately from the head at mild room temperatures, include this in your description when requesting a 25(OH)D test.
Vitamin D receptors are expressed in over 30 tissues — which is why deficiency produces such a diverse symptom picture. The 11 signs above are listed in order of frequency in deficient adults over 60. Most deficient seniors experience 3-5 of these simultaneously. None is specific enough to diagnose deficiency alone — a 25(OH)D blood test is required for confirmation.
Symptoms by System — The Clustering Pattern
One of the most useful clinical patterns in vitamin D deficiency is symptom clustering. Individual symptoms are non-specific, but three or more from different body systems appearing simultaneously makes deficiency significantly more probable:
Symptom cluster
Body systems affected
Probability of deficiency
Action
Fatigue + bone ache + muscle weakness
Energy, skeletal, muscular
High — classic triad
Request 25(OH)D blood test immediately
Low mood + brain fog + fatigue
Neurological, energy
Moderate — assess alongside thyroid
Request 25(OH)D and TSH together
Frequent illness + slow wound healing
Immune, skin
Moderate — assess alongside iron and B12
Request 25(OH)D, ferritin, B12
Hair thinning + fatigue + low mood
Dermatological, energy, neurological
Moderate — common in women post-menopause
Request 25(OH)D, ferritin, thyroid panel
Back pain + hip pain + muscle weakness
Skeletal, muscular
High — particularly in women over 65
Request 25(OH)D and DEXA scan
Single symptom only
One system
Low — many other causes
Start with 25(OH)D if other causes excluded
How to Test for Vitamin D Deficiency — What Your Results Mean
The Test
The correct test is 25-hydroxyvitamin D (written as 25(OH)D or calcidiol). This measures your storage vitamin D levels — the form that reflects dietary intake and skin synthesis. It is available through any standard blood panel and is often included in annual wellness bloodwork. If your physician has not ordered it, request it specifically.
Do not confuse this with 1,25-dihydroxyvitamin D (calcitriol) — the active hormone form. This test reflects immediate vitamin D activity and is not an accurate marker of overall vitamin D status. Always request 25(OH)D specifically.
Interpreting Your Results
25(OH)D level
Classification
What it means
Recommended action
Below 12 ng/mL (30 nmol/L)
Severe deficiency
Clinical deficiency — bone and immune function significantly impaired
Physician-supervised correction — typically 50,000 IU weekly for 8-12 weeks then maintenance
12–20 ng/mL (30–50 nmol/L)
Deficiency
Common in seniors — bone, muscle, immune, and mood effects likely
Start 4,000 IU D3 daily with meals; retest at 3 months
20–29 ng/mL (50–72 nmol/L)
Insufficiency
Below optimal for seniors — muscle, immune, and cardiovascular protection suboptimal
Start 2,000 IU D3 daily; retest at 3 months
30–39 ng/mL (75–97 nmol/L)
Adequate
NIH adequate threshold — bone protection sufficient
Maintain with 1,000–2,000 IU daily
40–60 ng/mL (100–150 nmol/L)
Optimal for seniors
Endocrine Society recommended range for adults over 60
Maintain current supplementation — retest annually
Above 80 ng/mL (200 nmol/L)
Potentially excessive
Above therapeutic range — reduce dose
Reduce supplementation; physician review
⚠️ Important — The 1,000 IU Myth Many adults over 60 are supplementing with only 600–1,000 IU of vitamin D daily from their multivitamin and believe they are protected. They are usually not. Population studies consistently show that 1,000 IU daily is insufficient to raise 25(OH)D levels to the 40–60 ng/mL optimal range in the majority of seniors — particularly those over 70, darker-skinned adults, and those spending significant time indoors. Get your level tested before assuming any particular dose is adequate.
Adults over 70 — skin synthesis declines most sharply in the seventh decade and beyond
Seniors with limited sun exposure — those who are housebound, in care facilities, or live above 35 degrees latitude in winter
Darker skin tones — melanin reduces vitamin D synthesis efficiency by 50–90%
Obese seniors — vitamin D is fat-soluble and becomes sequestered in adipose tissue, reducing circulating levels
Seniors on corticosteroids (prednisone) — accelerate vitamin D catabolism
Those with fat malabsorption — Crohn’s, coeliac disease, post-bariatric surgery
Seniors on certain medications — anticonvulsants, rifampicin, some antiretrovirals reduce vitamin D levels
Those taking PPIs long-term — impairs the gut environment for fat-soluble vitamin absorption
What to Do If You Are Deficient
Step 1 — Choose the Right Form
Always choose vitamin D3 (cholecalciferol) — not D2 (ergocalciferol). Multiple clinical trials confirm D3 is 87% more potent per unit than D2 and maintains blood levels more effectively after supplementation stops. Virtually all quality vitamin D supplements now use D3.
Based on your test result and the table above, select a corrective dose. The most commonly needed starting dose for deficient adults over 60 is 2,000–4,000 IU daily. Always take with your largest fat-containing meal — fat increases absorption by approximately 50%.
Step 3 — Add K2
At doses of 2,000 IU or above, always pair D3 with vitamin K2 MK-7 (90–180mcg daily). D3 increases intestinal calcium absorption — without K2 to direct that calcium into bone rather than arterial walls, high-dose D3 supplementation carries a theoretical cardiovascular calcification risk. The K2 pairing is now standard guidance in functional medicine and is increasingly recommended by cardiologists.
Magnesium is required as a cofactor for the enzymatic conversion of storage vitamin D to its active hormone form — deficiency in both simultaneously (affecting roughly 42% and 48% of US adults respectively) means D3 supplementation will be partially ineffective until magnesium is also corrected. For the complete magnesium guide including the best forms for seniors: 5 Best Magnesium Supplements for Seniors — Ranked by Form and Use Case.
Request a repeat 25(OH)D test 3 months after starting supplementation to confirm your levels have reached the 40–60 ng/mL target range. Many seniors need dose adjustments — particularly those who are obese, have fat malabsorption, or started from severely deficient levels. Annual retesting thereafter is appropriate to confirm maintained adequacy.
Step 5 — Address the Magnesium Co-factor
Vitamin D conversion to its active hormone form requires magnesium as a cofactor. Approximately 48% of US adults are deficient in magnesium — meaning that vitamin D supplementation may be partially ineffective if magnesium deficiency is also present. If you are correcting vitamin D deficiency and not seeing the expected symptom improvement, assess magnesium status and consider supplementing magnesium glycinate 200–300mg daily alongside D3.
Magnesium is required as a cofactor for the enzymatic conversion of storage vitamin D to its active hormone form — deficiency in both simultaneously (affecting roughly 42% and 48% of US adults respectively) means D3 supplementation will be partially ineffective until magnesium is also corrected. For the complete magnesium guide including the best forms for seniors: 5 Best Magnesium Supplements for Seniors — Ranked by Form and Use Case.
If you begin D3 supplementation at an appropriate corrective dose and symptoms persist after 3 months, consider these four explanations before concluding D3 is not helping:
Your magnesium is also low — D3 cannot be activated without adequate magnesium; supplement magnesium glycinate 200–300mg daily alongside D3
Your dose is insufficient — retest at 3 months to confirm your level has reached 40–60 ng/mL; if not, the dose needs to increase
You have fat malabsorption — vitamin D is fat-soluble and will not absorb properly if you have GI conditions that impair fat absorption; consider a water-soluble D3 preparation
The symptoms have a different primary cause — fatigue, muscle weakness, and bone pain have many other causes; if D3 correction to adequate levels does not produce significant improvement, pursue other investigations including thyroid function, B12, iron, and rheumatological assessment
What are the first signs of vitamin D deficiency in seniors?
The earliest and most common signs are persistent fatigue that does not resolve with rest, a diffuse aching in the bones (particularly lower back and legs), and increased susceptibility to infections. These three symptoms together — fatigue, bone ache, and frequent illness — form the classic early triad of vitamin D deficiency in older adults. They are almost universally attributed to normal aging, which is why deficiency goes undetected for years in the majority of affected seniors. The only way to confirm is a 25-hydroxyvitamin D blood test.
Can low vitamin D cause extreme fatigue in seniors?
Yes — fatigue is the most consistently reported symptom of vitamin D deficiency in older adults. The mechanism is direct: vitamin D regulates genes involved in mitochondrial energy production in skeletal and cardiac muscle. Without adequate D3, cellular ATP production is impaired at a fundamental level — producing the characteristic fatigue that persists regardless of sleep quality. In multiple clinical trials, vitamin D correction at 2,000–4,000 IU daily has produced significant improvement in fatigue scores within 4–8 weeks in deficient adults.
How long does it take for vitamin D supplements to work for deficiency symptoms?
Timeline varies by symptom and severity of deficiency. Fatigue and mood improvements typically begin within 4–8 weeks of corrective supplementation. Muscle strength improvements are measurable at 8–12 weeks. Bone pain from osteomalacia (severe deficiency) may take 3–6 months to fully resolve as bone mineralisation catches up. Immune function improvements — reduced illness frequency — are typically noticeable within one respiratory illness season (3–4 months). Get a repeat 25(OH)D blood test at 3 months to confirm your levels have reached the 40–60 ng/mL optimal range, as dose adjustments may be needed.
What vitamin D level is considered deficient for seniors?
The NIH defines deficiency as below 20 ng/mL (50 nmol/L) for bone health purposes. However, many vitamin D researchers and the Endocrine Society recommend a higher threshold of 30 ng/mL for sufficiency in older adults, with an optimal range of 40–60 ng/mL for adults over 60 to support muscle function, immune health, cardiovascular health, and cognitive function beyond just bone protection. Many seniors supplementing at 600–1,000 IU from their multivitamin fall in the 20–30 ng/mL insufficient range — technically not deficient by strict criteria but below the level associated with optimal function in older adults.
Can you get enough vitamin D from sunlight after 60?
For most seniors, no. Skin synthesis efficiency declines approximately 75% between ages 20 and 70. A 70-year-old spending 30 minutes in midday summer sun produces approximately 25% of the vitamin D that the same exposure would produce in a 25-year-old. Additionally, most seniors have more skin covered, use sunscreen more consistently, and spend less time outdoors than younger adults. Darker skin tones further reduce synthesis efficiency. Sensible sun exposure contributes modestly — but cannot substitute for daily D3 supplementation in adults over 60 living above 35 degrees latitude or spending significant time indoors.
Does vitamin D deficiency cause muscle pain or joint pain?
Vitamin D deficiency causes muscle weakness (particularly proximal muscles — thighs, hips, shoulders) and deep bone aches — not joint pain in the articular sense. The distinction matters: arthritis causes pain at the joint itself (the knee joint, hip socket, finger joints), while vitamin D deficiency produces a diffuse aching in the shaft of the bone and general muscle weakness. Many seniors have both conditions simultaneously — which is why vitamin D assessment is valuable even in seniors with confirmed arthritis, since deficiency can amplify pain perception and impair the muscle support that protects arthritic joints.
Can low vitamin D cause brain fog in seniors?
Yes — and the mechanism is direct, not speculative. Vitamin D receptors are expressed throughout the brain including the hippocampus, prefrontal cortex, and cingulate cortex — regions governing memory, executive function, and sustained attention. Deficiency impairs the expression of neuroprotective genes, reduces amyloid clearance efficiency, and increases neuroinflammation through microglial activation. Many seniors report a significant improvement in mental clarity — faster word retrieval, better sustained concentration, reduced mental fatigue — within 4–8 weeks of correcting deficiency to the 40–60 ng/mL optimal range. If you have been experiencing brain fog that has worsened over 1–2 years, a 25(OH)D blood test is one of the first investigations worth completing before attributing the change to normal cognitive aging.
Why do bones ache more at night with vitamin D deficiency?
When vitamin D is chronically low, the body increases parathyroid hormone (PTH) production to maintain blood calcium levels. Elevated PTH stimulates osteoclasts — the cells that break down bone — to release calcium from the bone matrix into the bloodstream. This process of high bone turnover generates inflammatory signals within the bone tissue itself. The aching sensation is most noticeable at night and at rest because the physical distractions of daytime activity mask the pain signal, which becomes perceptible when the body is still and quiet. The pain is characteristically deep within the bone shaft — in the tibia, femur, lower back, and ribs — rather than at the joint surfaces where arthritis pain localises.
Can I get enough vitamin D from a standard multivitamin?
For most seniors over 60, no. Standard multivitamins contain 400–1,000 IU of vitamin D — formulated to the RDA which was established to prevent rickets and osteomalacia in the general population, not to maintain the 40–60 ng/mL blood levels associated with optimal muscle function, immune response, and cognitive protection in older adults. Population data consistently shows that 1,000 IU daily is insufficient to raise 25(OH)D levels above 30 ng/mL in the majority of seniors — particularly those over 70, those with darker skin tones, obese individuals, and those spending limited time outdoors. Most seniors require 2,000–4,000 IU daily to maintain the 40–60 ng/mL optimal range. Get your level tested before assuming any particular dose is adequate.
Does vitamin D deficiency cause weight gain in seniors?
Indirectly yes — through two mechanisms. First, vitamin D is fat-soluble and becomes sequestered in adipose tissue, meaning that weight gain reduces circulating vitamin D levels and worsens deficiency in a self-reinforcing cycle. Second, vitamin D deficiency impairs fast-twitch muscle fibre function, reducing the capacity for physical activity and accelerating the muscle loss (sarcopenia) that slows metabolic rate in older adults. Correcting vitamin D deficiency will not directly cause weight loss, but it removes two metabolic barriers — reduced physical capacity and impaired muscle function — that otherwise work against healthy weight maintenance after 60.
What foods have the most vitamin D for seniors?
The dietary vitamin D sources with meaningful content are: fatty fish (salmon 3oz provides approximately 570 IU, mackerel 360 IU, sardines 165 IU), egg yolks (approximately 40 IU per yolk), and fortified foods (most US dairy milk provides 120 IU per cup, some fortified orange juices 100 IU per cup). The practical reality for seniors: even an excellent diet rich in fatty fish and fortified dairy provides only 400–600 IU daily — well below the 2,000 IU most seniors need. Dietary sources are valuable as a contribution but cannot substitute for direct supplementation in adults over 60 with the skin synthesis limitations of aging.
How is vitamin D deficiency different from vitamin D insufficiency?
Deficiency is typically defined as 25(OH)D below 20 ng/mL (50 nmol/L) — the threshold at which bone health, immune function, and muscle function are significantly impaired. Insufficiency is 20–29 ng/mL — where bone protection is adequate but the broader functions of vitamin D in muscle, cardiovascular, immune, and neurological health are suboptimal for adults over 60. The practical distinction: deficiency produces the more obvious symptoms described in this article — bone pain, pronounced muscle weakness, severe fatigue. Insufficiency produces subtler symptoms that are even easier to attribute to normal aging — reduced stamina, slightly increased illness frequency, lower mood — but that still respond significantly to optimising levels to 40–60 ng/mL.
The Bottom Line
Vitamin D deficiency is the most underdiagnosed correctable health condition in adults over 60. The 11 symptoms described in this guide — from fatigue and bone ache to low mood and brain fog — are almost universally attributed to normal aging. They are, in roughly half of all cases, partly or entirely driven by a deficiency that a blood test can confirm and daily supplementation can correct.
The single most important action: request a 25-hydroxyvitamin D blood test. If your level is below 30 ng/mL, start D3 at 2,000–4,000 IU daily with your largest meal, paired with K2 MK-7 90–180mcg, and retest at 3 months. The cost is approximately $0.03–0.10 per day. The potential benefit — restored energy, reduced bone pain, improved muscle strength, better mood, and lower fall and infection risk — is among the highest ROI health interventions available to seniors.
If you have already been diagnosed with vitamin D deficiency and are supplementing but not seeing symptom improvement, check magnesium status — D3 cannot be activated without magnesium, and 48% of US adults are magnesium deficient simultaneously.



")