⚕️ Medical Disclosure — Read Before Starting Berberine Berberine Supplement for Seniors has clinically significant blood glucose-lowering effects and MUST be disclosed to any physician managing diabetes or prediabetes before starting. In seniors taking diabetes medications (metformin, insulin, sulfonylureas such as glipizide or glimepiride), berberine can cause hypoglycaemia — blood sugar dropping dangerously low. Berberine is also a significant CYP3A4 liver enzyme inhibitor and CYP2D6 inhibitor, meaning it slows the metabolism of many prescription medications and raises their blood levels. Run your complete medication list past your pharmacist before starting berberine. This is not a mild caution — the drug interaction risk is real and potentially serious. This article does not constitute medical advice.
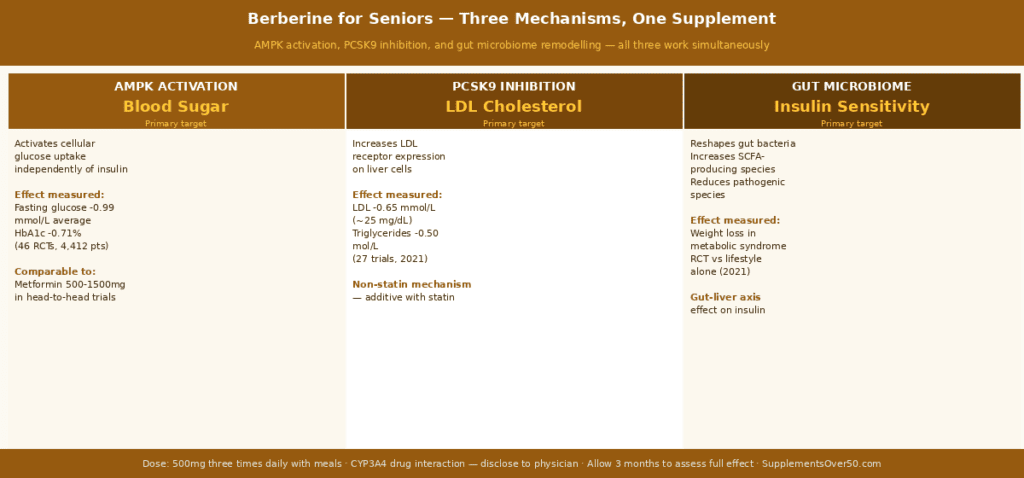
⚡ Quick Answer Berberine is an alkaloid derived from Berberis plants (barberry, goldenseal, Oregon grape) with three clinically validated mechanisms relevant to senior metabolic health: AMPK activation (mimics exercise-like cellular glucose uptake independent of insulin), PCSK9 inhibition (reduces LDL cholesterol through a non-statin pathway), and gut microbiome remodelling (improves insulin sensitivity through the gut-liver axis). A 2023 meta-analysis of 46 RCTs confirmed berberine significantly reduces fasting blood glucose, HbA1c, total cholesterol, LDL, and triglycerides in adults with metabolic syndrome. Standard dose: 500mg three times daily with meals. Expect 3 months for full effect assessment. Drug interaction risk is significant — always disclose to your physician and pharmacist.
Why Berberine Supplement for Seniors is Particularly Relevant After 60
The metabolic changes of aging after 60 create a specific pattern that berberine’s three mechanisms directly address. Understanding why requires understanding what changes in metabolic physiology as we age — because berberine is not a generic ‘wellness supplement.’ It has specific biological targets that happen to align closely with the metabolic dysfunction pattern of normal aging.
The Post-60 Metabolic Shift
Four converging changes characterise the metabolic trajectory of most adults after 60, even those eating well and exercising regularly. First, insulin resistance increases in muscle tissue — muscle cells develop reduced sensitivity to insulin-mediated glucose uptake, meaning more insulin is required to clear the same amount of glucose from the bloodstream. This manifests as the gradual upward creep of fasting blood glucose that many adults over 60 notice on their annual blood panels.
Second, AMPK (AMP-activated protein kinase) activity declines. AMPK is the master metabolic sensing enzyme — the cellular switch that detects the ratio of AMP to ATP (energy depletion signal versus energy abundance signal) and responds by stimulating glucose uptake, fatty acid oxidation, and mitochondrial biogenesis. Regular vigorous exercise is the most potent natural AMPK activator. As both AMPK baseline activity and exercise capacity decline with age, the cellular mechanisms that maintain metabolic efficiency weaken simultaneously.
Third, hepatic cholesterol synthesis becomes less regulated. The liver’s internal feedback mechanisms that match cholesterol production to need become less responsive, and PCSK9 — the enzyme that degrades LDL receptors on liver cells — becomes more active. Fewer LDL receptors means less LDL clearance from the bloodstream, contributing to the LDL elevation that many adults first notice in their 50s and 60s.
Fourth, triglycerides accumulate. Reduced fat oxidation efficiency (from declining AMPK activity), increased hepatic fat synthesis in the context of insulin resistance, and the dietary fat landscape typical of Western eating patterns combine to elevate fasting and postprandial triglycerides — a cardiovascular risk factor that becomes increasingly significant in older adults relative to younger ones.
Berberine addresses all four of these simultaneously through overlapping but distinct mechanisms. This is why it has attracted more serious scientific attention than most supplements — its clinical profile looks less like a nutraceutical and more like a metabolic medication.
Key Statistics — The Evidence Base
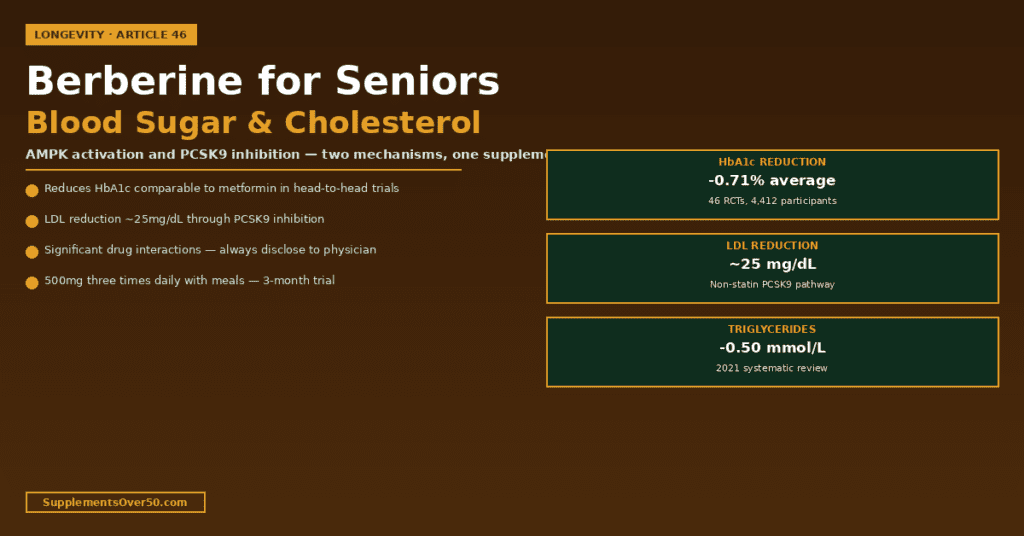
A 2023 meta-analysis of 46 RCTs involving 4,412 participants confirmed berberine significantly reduces fasting blood glucose by an average of 0.99 mmol/L (approximately 18 mg/dL), HbA1c by 0.71%, and fasting insulin by 2.33 mU/L compared to placebo or active comparators
A 2021 systematic review of 27 trials found berberine reduced LDL cholesterol by an average of 0.65 mmol/L (approximately 25 mg/dL), total cholesterol by 0.61 mmol/L, and triglycerides by 0.50 mmol/L
Head-to-head trials comparing berberine 500mg three times daily versus metformin 500mg three times daily found comparable glucose-lowering efficacy, with berberine showing similar or slightly superior lipid improvements and better GI tolerability in some studies
Berberine reduces body weight by an average of 2.3 kg and waist circumference by 2.1 cm in adults with metabolic syndrome in RCTs — attributed primarily to its effects on gut microbiome composition and insulin sensitisation
Berberine’s PCSK9 inhibition mechanism is independent of the HMG-CoA reductase pathway targeted by statins — making it potentially additive with statin therapy rather than redundant
A 2022 study found berberine reduces hsCRP (high-sensitivity C-reactive protein) — a marker of systemic inflammation — significantly in adults with metabolic syndrome, suggesting anti-inflammatory effects beyond its direct metabolic actions
How Berberine Works — The Three Mechanisms in Detail
Mechanism 1 — AMPK Activation: The Exercise Mimetic Effect
AMP-activated protein kinase (AMPK) is the cell’s master energy sensor. When cellular energy reserves are low (high AMP:ATP ratio — as happens during exercise), AMPK activates a coordinated response: GLUT4 glucose transporters move to the cell surface allowing insulin-independent glucose uptake, fatty acid oxidation accelerates, and mitochondrial biogenesis is stimulated. AMPK activation is one of the primary reasons exercise improves metabolic health — it is the molecular mechanism behind exercise’s blood sugar-lowering effect.
Berberine activates AMPK through a different route — by mildly inhibiting mitochondrial Complex I in the electron transport chain. This creates a modest and temporary reduction in ATP production that the cell detects as an energy-low signal, triggering AMPK activation as a compensatory response. The net effect mimics an exercise-like metabolic state in cells: more glucose is taken up independently of insulin, fatty acid oxidation increases, and the downstream metabolic improvements associated with regular exercise occur at the cellular level.
This is why berberine and metformin have overlapping effects — metformin also activates AMPK through Complex I inhibition. The mechanisms are not identical (berberine has additional targets) but they share this fundamental pathway, which is why head-to-head trials show comparable glucose-lowering efficacy.
The practical implication for seniors: berberine provides AMPK-mediated metabolic benefit that partially compensates for the declining exercise capacity and declining baseline AMPK activity that characterise normal aging. For a senior who cannot exercise at the intensity required to generate significant AMPK activation, berberine provides a complementary metabolic benefit through the same cellular pathway.
Mechanism 2 — PCSK9 Inhibition: The Non-Statin LDL Reducer
PCSK9 (proprotein convertase subtilisin/kexin type 9) is a liver enzyme that binds to LDL receptors on hepatocyte surfaces and tags them for degradation. The more PCSK9 activity, the fewer LDL receptors survive on liver cells, and the less LDL is cleared from the bloodstream. This pathway is so important to cardiovascular medicine that pharmaceutical PCSK9 inhibitors (evolocumab/Repatha and alirocumab/Praluent) are among the most expensive and effective LDL-lowering drugs available — reducing LDL by 50-60% in high-risk patients.
Berberine inhibits PCSK9 expression at the transcriptional level — it reduces how much PCSK9 the liver produces, which allows more LDL receptors to survive and clear more LDL from circulation. The effect is substantially smaller than pharmaceutical PCSK9 inhibitor drugs (25 mg/dL average LDL reduction versus 60-100 mg/dL for drugs) but operates through a completely different pathway from statins. This is clinically significant for two reasons.
First, berberine’s LDL reduction is additive with statin therapy because it uses a different mechanism. A statin inhibits cholesterol synthesis upstream; berberine increases LDL clearance downstream. The combination can produce greater total LDL reduction than either alone — relevant for seniors whose LDL is not adequately controlled on their current statin dose but who want to avoid dose escalation due to side effect concerns.
Second, seniors with LDL elevations who want to avoid statins entirely — due to muscle pain (myalgia), cognitive concerns, or personal preference — have in berberine the best-evidenced non-statin alternative for LDL management, with a mechanism that addresses the same receptor pathway targeted by the most expensive cardiovascular drugs in current use.
Mechanism 3 — Gut Microbiome Remodelling: The Insulin Sensitivity Pathway
The gut microbiome’s influence on metabolic health operates through the gut-liver axis — the signalling pathway between intestinal bacteria, their metabolic products, and hepatic glucose and fat metabolism. Short-chain fatty acids (SCFAs) produced by beneficial bacteria (particularly Bifidobacterium and Faecalibacterium prausnitzii) improve insulin sensitivity by activating GPR41/43 receptors in the gut wall and liver, reducing hepatic gluconeogenesis, and increasing GLP-1 secretion.
In adults with metabolic syndrome and insulin resistance, gut microbiome dysbiosis is consistently observed: beneficial SCFA-producing bacteria are depleted, and pathogenic species associated with endotoxemia and insulin resistance are enriched. Lipopolysaccharide (LPS) from gram-negative bacterial cell walls leaks through a disrupted gut barrier into portal circulation, triggering hepatic inflammation that directly worsens insulin resistance.
Berberine reshapes the gut microbiome in a direction that improves metabolic function: it selectively inhibits pathogenic gram-negative species (reducing endotoxin production) while supporting beneficial bacterial populations. A 2020 study confirmed berberine-treated adults showed significantly increased Bifidobacterium and Lactobacillus populations alongside improved insulin sensitivity compared to placebo. This gut-mediated mechanism is distinct from AMPK activation and contributes additional metabolic benefit beyond what AMPK alone would predict — explaining why berberine’s observed effects in large meta-analyses are sometimes larger than models based purely on its direct cellular actions would suggest.
Berberine addresses the post-60 metabolic pattern through three non-overlapping mechanisms simultaneously. AMPK activation mirrors the metabolic benefit of exercise at the cellular level. PCSK9 inhibition provides non-statin LDL reduction additive with statin therapy. Gut microbiome remodelling contributes additional insulin sensitisation through the gut-liver axis.
Berberine vs Metformin — The Comparison Seniors Are Asking About
Berberine’s comparison to metformin is one of the most discussed topics in metabolic supplement research. The comparison is clinically meaningful because both drugs target overlapping pathways — but they are not the same, and the comparison has important nuances for seniors deciding how to manage prediabetes or mildly elevated LDL.
Factor
Berberine 500mg three times daily
Metformin 500–2,000mg daily
Mechanism
AMPK activation + PCSK9 inhibition + gut microbiome remodelling
AMPK activation + reduced hepatic glucose production (primary)
Blood glucose reduction
Comparable in head-to-head trials — average FBG -0.99 mmol/L in meta-analysis
Well-established; -1.0 to -1.5 mmol/L FBG in most trials
HbA1c reduction
Average -0.71% across 46 RCTs
Average -0.9 to -1.2% in established diabetes trials
LDL cholesterol
-0.65 mmol/L (~25 mg/dL) via PCSK9 inhibition
Minimal — not a primary metformin action
Triglycerides
-0.50 mmol/L average
Modest reduction in some studies
Weight
Average -2.3 kg in metabolic syndrome RCTs
Modest — typically 1-3 kg in long-term use
Prescription required
No — dietary supplement
Yes — prescription medication in US/Canada
GI side effects
Nausea, constipation (start low and slow)
Nausea, diarrhoea common — GI-limiting in 20-30% of users
B12 depletion
No known B12 depletion
Yes — metformin significantly depletes B12 over time; requires monitoring
Drug interactions
Significant — CYP3A4 and CYP2D6 inhibitor
Moderate — fewer significant interactions
Cancer risk data
Emerging evidence for cancer-protective effects (AMPK)
Long-term data shows reduced cancer incidence vs no treatment
Not typically prescribed in US/Canada without diabetes diagnosis
Best for seniors with diabetes
Adjunct to physician management — not replacement
First-line medication for type 2 diabetes under physician care
The practical conclusion for seniors: berberine is not a substitute for metformin in diagnosed type 2 diabetes — metformin has decades of safety data, mortality benefit data, and physician oversight. However, for seniors with prediabetes (fasting glucose 100-125 mg/dL or HbA1c 5.7-6.4%), mildly elevated LDL, or metabolic syndrome who want a non-prescription metabolic intervention with the strongest available clinical evidence, berberine is the most compelling option available.
⚠️ Critical Drug Interaction Warning — Read Before Starting Berberine inhibits CYP3A4 and CYP2D6 — two of the most important liver enzymes responsible for metabolising prescription medications. Inhibiting these enzymes slows drug clearance, raising blood levels of affected medications to potentially dangerous levels. Medications significantly affected include: statins (simvastatin, lovastatin, atorvastatin — increased myopathy risk at elevated blood levels), cyclosporine and tacrolimus (immunosuppressants — narrow therapeutic window), certain antibiotics (clarithromycin, erythromycin), some antifungals (ketoconazole), calcium channel blockers (amlodipine, diltiazem, verapamil), and some antidepressants metabolised by CYP2D6. This is not a theoretical concern — it is a clinically validated pharmacokinetic interaction. Before starting berberine, provide your complete medication list to your pharmacist and ask specifically about CYP3A4 and CYP2D6 interactions with your current medications.
Dosing Protocol for Seniors — Starting Safely
The standard therapeutic dose used in the majority of positive clinical trials is 500mg three times daily with meals (1,500mg total daily). However, this dose should not be the starting dose for most seniors — particularly those on multiple medications or with any history of GI sensitivity. A gradual introduction reduces both GI side effects and the risk of drug interactions becoming apparent too quickly to manage safely.
Week 1-2 — Test Dose
Start with 250mg once daily with your largest meal. This sub-therapeutic starting dose establishes GI tolerability and allows your physician to check for any interaction signals if you are on relevant medications. Most seniors experience no side effects at this dose. Common GI side effects — mild nausea, constipation, or bloating — usually appear within the first few days at higher doses and resolve with dose reduction.
Week 3-4 — Step Up
Increase to 250mg twice daily — once with breakfast and once with dinner. Blood glucose monitoring (if relevant) should begin here as the glucose-lowering effect becomes physiologically meaningful at this dose. Seniors on blood pressure medication should check their blood pressure readings weekly during this phase as berberine’s mild vasodilatory effect may add to antihypertensive drug effects.
Week 5-6 — Therapeutic Dose
Increase to 500mg twice daily (1,000mg total). Some protocols use 500mg three times daily for the full 1,500mg dose — the additional benefit of the third dose over two doses is modest and the two-dose protocol is simpler and generally better tolerated. Clinical trials showing significant metabolic benefits have used both two and three-dose protocols.
Month 3 — Assessment
Retest fasting blood glucose, HbA1c, and fasting lipid panel (LDL, triglycerides, total cholesterol) at 3 months. These are the objective measures that tell you whether berberine is working for your specific metabolism. Expected changes: fasting glucose reduction of approximately 10-20 mg/dL, HbA1c reduction of 0.5-0.8%, LDL reduction of 15-25 mg/dL, and triglyceride reduction of 15-30 mg/dL. If changes are within these ranges, the supplement is working as expected.
Goal
Starting dose
Maintenance dose
Timing
Assessment timeframe
Blood glucose management (prediabetes)
250mg once daily with largest meal for 2 weeks
500mg twice daily with breakfast and dinner
Always with meals — significantly reduces GI effects
3 months — retest FBG and HbA1c
LDL/cholesterol reduction
250mg once daily
500mg twice or three times daily
With meals
3 months — retest fasting lipid panel
Full metabolic syndrome protocol
250mg once daily x 2 weeks
500mg three times daily
With each of three main meals
3 months — full metabolic panel
As statin complement
Discuss with physician first — CYP interaction with statins
Physician-guided dose
Physician-guided timing
Monthly monitoring during titration
Who Should Not Take Berberine
Despite its evidence base, berberine is not appropriate for all seniors. The following groups should avoid berberine or use only under physician supervision:
Pregnant or breastfeeding women — berberine crosses the placenta and may cause neonatal jaundice; not relevant for seniors but included for completeness
Stage 3+ chronic kidney disease — berberine and its metabolites are renally excreted; impaired kidney function may lead to accumulation
Significant liver disease — berberine is hepatically metabolised and may further burden an already compromised liver
Seniors on anticoagulants (warfarin, Eliquis, Xarelto) — CYP3A4 inhibition can raise anticoagulant blood levels, increasing bleeding risk; requires INR monitoring if used
Seniors on narrow therapeutic index medications including cyclosporine, tacrolimus, digoxin, or certain antiseizure medications — the CYP interaction profile makes these combinations genuinely hazardous without physician monitoring
Seniors with hypoglycaemia risk — those with reactive hypoglycaemia or on insulin should monitor blood glucose closely as berberine’s AMPK activation adds to glucose-lowering effects
Berberine and Blood Sugar — Practical Monitoring for Seniors
For seniors using berberine specifically for prediabetes management, a structured monitoring protocol ensures both safety and effectiveness assessment:
Week 2: First blood glucose check after reaching 500mg daily dose — looking for unexpected hypoglycaemia particularly if on other glucose-lowering agents
Month 1: Blood pressure check and symptom review — nausea, constipation, muscle symptoms (relevant if on statin)
Month 6: Repeat metabolic panel — confirms sustained benefit and monitors for any long-term liver enzyme changes
If fasting blood glucose drops below 70 mg/dL at any point — lightheadedness, shakiness, sweating, confusion — reduce the berberine dose immediately and contact your physician. Hypoglycaemia is not a typical berberine side effect in non-diabetic adults but can occur in those with borderline glucose regulation or concurrent glucose-lowering medications.
Berberine Forms and Products — What to Look For
Standard Berberine HCl
The majority of clinical trials used berberine hydrochloride (HCl) — the most widely available and most affordable form. Berberine HCl has limited oral bioavailability (approximately 5% absorption in standard tablet form) due to poor aqueous solubility. This is partly why three-times-daily dosing is used — smaller, more frequent doses improve total absorption compared to a single large dose.
Berberine phytosome (Berbevis or similar branded extracts) complexes berberine with phosphatidylcholine, dramatically improving absorption. Studies comparing berberine phytosome to standard HCl found 3-5 times higher berberine blood levels from equivalent doses. This means the phytosome form may produce comparable clinical effects at approximately half the dose of standard berberine HCl — potentially reducing GI side effects at the therapeutic level. Best products using this technology: Thorne Berberine-500 and Life Extension Berberine Fasting Support.
Dihydroberberine (DHB)
Dihydroberberine is a reduced form of berberine produced naturally in the gut from berberine by intestinal bacteria. DHB absorbs approximately 5 times more efficiently than standard berberine HCl and converts back to berberine in intestinal cells. GlucoVantage is the primary branded DHB ingredient. Several small trials suggest equivalent or superior clinical effects at lower doses with significantly reduced GI side effects. This is the highest-bioavailability berberine option but commands a significant price premium. Best for: seniors who experience GI intolerance with standard berberine HCl at therapeutic doses.
Form
Relative bioavailability
Typical effective dose
Cost per day
GI tolerance
Berberine HCl
Standard (1x)
500mg three times daily
~$0.20-0.35
Moderate — nausea and constipation at higher doses
500mg berberine HCl per capsule with NSF Certified manufacturing. One of the few berberine products with certified GMP manufacturing at the level expected for pharmaceutical-grade supplements. ~$0.60/day for 500mg twice daily. Best for seniors who prioritise manufacturing quality and third-party certification.
2. Life Extension Berberine Glucose Support — Amazon / iHerb — Best Value with Added Ingredients
500mg berberine HCl with silymarin (milk thistle) for liver support — a thoughtful formulation given berberine’s hepatic metabolism. ~$0.35-0.45/day. Best for seniors wanting the berberine-liver support combination.
3. NOW Berberine 400mg — Amazon / Walmart — Best Budget Option
400mg berberine HCl per capsule. Well-reviewed, widely available at Walmart for in-store access. ~$0.20-0.25/day at three capsules daily. Best for budget-conscious seniors who want to try berberine at low cost before committing to premium forms.
4. Thorne GlucoVantage (Dihydroberberine) — Thorne.com — Best for GI-Sensitive Seniors
100mg dihydroberberine (DHB) per capsule using GlucoVantage branded extract — approximately equivalent to 500mg standard berberine HCl at 5x absorption. ~$0.60-0.80/day at two capsules. Best for seniors who experienced GI intolerance with standard berberine.
5. Integrative Therapeutics Berberine Complex — Amazon — Best Combination Formula
500mg berberine HCl with alpha lipoic acid and chromium — addressing insulin sensitivity through complementary mechanisms. ~$0.55-0.70/day. Best for seniors managing prediabetes who want a multi-ingredient metabolic support approach.
Berberine and the Broader Senior Cardiovascular Stack
For seniors using berberine as part of a comprehensive cardiovascular and metabolic health approach, the supplement combinations that work well together without negative interactions are worth mapping:
Berberine + Omega-3 EPA+DHA: strong combination — omega-3 reduces triglycerides through a different mechanism (reducing hepatic VLDL synthesis) and adds cardiovascular anti-inflammatory benefit that berberine’s metabolic mechanisms do not directly address
Berberine + CoQ10 Ubiquinol: appropriate combination — berberine mildly inhibits mitochondrial Complex I, which theoretically could reduce CoQ10 regeneration; supplemental ubiquinol compensates for any such effect. Especially relevant for seniors on statins who are already adding CoQ10
Berberine + Magnesium: compatible — magnesium supports insulin receptor signalling through a different pathway and adds blood pressure benefit complementary to berberine’s metabolic improvements
Berberine + Statin: discuss with physician first — CYP3A4 inhibition can raise statin blood levels, increasing myopathy risk; some physicians manage this combination successfully at reduced statin doses, but pharmacist review is essential
Berberine + Red Yeast Rice: avoid without physician guidance — both have LDL-lowering effects and red yeast rice contains monacolin K (a natural statin); combining them raises similar concerns to berberine + prescription statin
Berberine can be appropriate for healthy seniors over 70 with normal kidney and liver function, but requires more careful management than for younger adults for three reasons. First, the CYP3A4 drug interaction risk is more significant in older adults who typically take more concurrent medications. Second, kidney function — relevant for berberine excretion — declines with age, and seniors over 70 with eGFR below 60 ml/min/1.73m2 should use berberine only under physician guidance. Third, the hypoglycaemia risk from berberine’s glucose-lowering effect adds to the general hypoglycaemia vulnerability that increases with age. For seniors over 70 taking no relevant prescription medications and managing prediabetes or mild lipid elevation, berberine at 500mg twice daily is a reasonable evidence-based option — start at 250mg daily and increase gradually while monitoring blood glucose and blood pressure.
How long does berberine take to work for blood sugar?
Blood sugar improvements typically become measurable within 4-8 weeks of consistent use at 500mg twice or three times daily. Fasting blood glucose reductions of 10-20 mg/dL are typically observable at 4 weeks. HbA1c reflects 3-month average blood glucose and requires the full 3-month trial to assess accurately — expect a 0.5-0.8% reduction in prediabetic or mildly diabetic adults. Lipid improvements (LDL reduction, triglyceride reduction) are typically measurable at 8-12 weeks. Get objective baseline measurements of fasting blood glucose, HbA1c, and fasting lipids before starting and retest the same panel at 3 months to accurately evaluate whether berberine is producing the expected metabolic response in your specific metabolism.
Can berberine replace a statin for cholesterol?
Berberine cannot directly replace a statin for seniors with established cardiovascular disease, LDL above 160 mg/dL, or documented high cardiovascular risk requiring significant LDL reduction. Statins have decades of hard cardiovascular endpoint data — mortality reduction, myocardial infarction prevention, stroke prevention — that berberine does not yet have. For seniors with mildly elevated LDL (130-160 mg/dL) who prefer to avoid statins due to myalgia, cognitive concerns, or personal preference, berberine at 500mg twice or three times daily combined with omega-3 EPA+DHA and dietary modification produces clinically meaningful LDL and triglyceride reduction through a non-statin pathway. The most interesting clinical application is combining berberine with a statin at a lower statin dose — the PCSK9 inhibition adds to the statin’s HMG-CoA reductase inhibition, potentially allowing lower statin doses with equivalent LDL control and reduced dose-dependent side effects.
Does berberine cause liver damage?
Standard berberine supplementation at 500mg three times daily has not been associated with liver damage in clinical trials — liver enzyme monitoring in published RCTs has not shown significant hepatotoxicity. However, berberine is hepatically metabolised through CYP3A4, and seniors with pre-existing liver disease or significantly elevated liver enzymes should use caution and physician guidance. The more relevant concern is berberine’s CYP3A4 inhibition raising blood levels of other hepatically-metabolised drugs to levels where those drugs cause liver stress. If you are taking any medication that requires liver metabolism — which includes the majority of prescription drugs — run your medication list past your pharmacist before starting berberine.
What is the best time of day to take berberine?
Always with meals — this is the single most important timing rule for berberine. Taking berberine with food serves three purposes: it significantly reduces the GI side effects (nausea, stomach discomfort) that are the most common reason seniors discontinue use; it allows berberine to be present in the gut when dietary carbohydrates are being digested and absorbed, maximising its glucose-buffering effect at the postprandial (post-meal) blood sugar peak; and food slows gastric emptying, giving berberine more contact time with the intestinal wall for absorption. For the standard two-dose protocol, breakfast and dinner are the most practical timing. For three-dose protocols, breakfast, lunch, and dinner. Never take berberine on an empty stomach — the GI side effects are substantially worse and absorption may paradoxically be reduced.
Can berberine and metformin be taken together?
Not without physician supervision — this combination requires careful management. Both berberine and metformin lower blood glucose through overlapping AMPK pathways, and combining them significantly increases hypoglycaemia risk in patients with diabetes. Additionally, berberine’s CYP3A4 inhibition may affect metformin’s renal clearance in some contexts. The combination is not categorically contraindicated — some physicians do manage patients on both — but it requires physician oversight, dose adjustment, and regular blood glucose monitoring. Seniors who are considering both should have this conversation explicitly with their diabetes physician rather than self-managing the combination.
Can I take berberine and metformin together?
This combination requires direct physician supervision and should never be self-managed. Both berberine and metformin activate AMPK through overlapping pathways — taking them together produces additive glucose-lowering that significantly increases hypoglycaemia risk in seniors, particularly those with any tendency toward low blood sugar. The practical signs of hypoglycaemia to watch for: lightheadedness, shakiness, sweating, confusion, or unusual hunger — any of which warrant immediate dose reduction and physician contact. Beyond the hypoglycaemia risk, berberine’s CYP3A4 inhibition may affect metformin’s renal clearance in some contexts. If your physician specifically wants to combine them — some do for additive metabolic benefit at reduced doses of each — blood glucose monitoring at least twice daily during the initial titration period is essential. Never initiate this combination independently.
Does berberine interact with statins?
Yes — this is one of the most clinically important drug interactions in the berberine category and the one most frequently overlooked by seniors managing their own supplements. Berberine is a significant CYP3A4 inhibitor — it slows the liver’s metabolism of statins that use this enzyme, particularly simvastatin, lovastatin, and atorvastatin. When CYP3A4 activity is reduced, statin blood levels rise above their intended therapeutic range, increasing the risk of myopathy (muscle pain and weakness) and in severe cases rhabdomyolysis (muscle breakdown). The interaction is dose-dependent — it is more significant at higher berberine doses and with statins that are heavily CYP3A4-dependent. If you take any statin and want to start berberine, run the specific combination past your pharmacist before starting and report any new muscle pain or weakness immediately. Some physicians manage this combination by reducing the statin dose — but this requires physician direction, not self-adjustment.
Why does berberine cause constipation or diarrhoea?
Standard berberine HCl has approximately 5% oral bioavailability — meaning 95% of each dose remains unabsorbed in the gut. This large unabsorbed fraction has direct effects on gut motility and the intestinal microbiome that produce inconsistent GI symptoms. Constipation (more common than diarrhoea at standard doses in seniors) results from berberine’s antimicrobial effect on certain gut bacteria that normally support motility. Diarrhoea occurs when the osmotic effect of unabsorbed berberine draws water into the colon. Both can be reduced by switching to a higher-bioavailability form. Berberine phytosome absorbs 3-5 times more efficiently than HCl — less unabsorbed berberine in the gut means significantly fewer GI effects at the equivalent therapeutic blood level. Dihydroberberine (DHB) absorbs approximately 5 times more efficiently and has the best GI tolerability profile. Starting at 250mg once daily with the largest meal and increasing gradually also prevents the GI effects that arise when a full therapeutic dose is started immediately.
Can berberine help with weight loss in seniors over 60?
Berberine produces modest but consistent weight reduction in adults with metabolic syndrome — an average of 2.3 kg and 2.1 cm waist circumference reduction in published RCTs. The mechanism is not appetite suppression — it is metabolic: AMPK activation increases fat oxidation, PCSK9-independent effects improve lipid handling, and gut microbiome remodelling reduces the endotoxin-driven hepatic inflammation that promotes visceral fat accumulation. The weight and waist reduction is most pronounced in seniors with insulin resistance and metabolic syndrome — those with normal metabolic parameters show smaller responses. Berberine is not a primary weight loss supplement and should not be positioned as one. Its weight effects are a secondary benefit of its primary metabolic actions. For seniors with post-menopausal abdominal fat driven by cortisol dysregulation, combining berberine with ashwagandha KSM-66 addresses both the insulin resistance driver and the cortisol-visceral adiposity driver simultaneously.
How does berberine affect the gut microbiome in seniors?
Berberine has one of the most well-characterised gut microbiome effects of any supplement. It selectively inhibits pathogenic gram-negative bacteria whose cell wall lipopolysaccharide (LPS) leaks through a disrupted gut barrier into portal circulation — this endotoxemia directly drives hepatic insulin resistance and systemic inflammation. Simultaneously, berberine’s antimicrobial profile spares and modestly promotes beneficial SCFA-producing bacteria including Bifidobacterium and Lactobacillus strains. The net effect is a shift toward a metabolically healthier microbiome that produces more short-chain fatty acids, activates GLP-1 receptors more effectively, and generates less inflammatory endotoxin. This gut-liver axis improvement is why berberine’s clinical effects are somewhat larger than AMPK activation alone would predict. Seniors already taking a Bifidobacterium-rich probiotic will find the two approaches complementary — berberine reduces the pathogenic competition that limits probiotic colonisation while the probiotic directly replenishes the beneficial species berberine’s microbiome remodelling supports.
Is berberine safe for seniors with prediabetes who are not yet on medication?
Berberine is arguably most appropriate for this exact population — seniors with prediabetes (fasting glucose 100-125 mg/dL or HbA1c 5.7-6.4%) who are not yet on medication and want to delay or prevent progression to type 2 diabetes without a prescription. The 2023 meta-analysis of 46 RCTs confirms clinically meaningful fasting glucose and HbA1c reductions at 500mg twice or three times daily. There are no medication interaction concerns in this group (assuming no concurrent diabetes medications), and the drug interaction profile is manageable with pharmacist review of other prescriptions. The practical protocol: confirm baseline fasting glucose and HbA1c before starting, begin at 250mg daily with the largest meal, increase to 500mg twice daily over 4-6 weeks, and retest the same blood panel at 3 months. If fasting glucose has returned to below 100 mg/dL and HbA1c to below 5.7%, the prediabetes has been pharmacologically corrected — a meaningful and measurable outcome from a non-prescription intervention.
The Bottom Line
Berberine is the most compelling metabolic supplement for adults over 60 not currently managed with diabetes medication. Its triple mechanism — AMPK activation, PCSK9 inhibition, and gut microbiome remodelling — addresses the primary metabolic dysfunctions of aging (insulin resistance, elevated LDL, triglyceride accumulation) simultaneously through pathways that have been extensively validated in published clinical research.
The drug interaction profile is the most important caveat and the one most frequently minimised in consumer berberine marketing. CYP3A4 and CYP2D6 inhibition is real and clinically significant — a pharmacist medication review before starting is not optional for any senior on prescription medications. This is not a reason to avoid berberine; it is a reason to manage it properly.
For the right senior — prediabetes with fasting glucose in the 100-125 mg/dL range, LDL drifting upward without reaching statin-indicated levels, or metabolic syndrome managed without prescription medication — berberine at 500mg twice daily represents the highest-evidence non-prescription metabolic intervention currently available. Start at 250mg with the largest meal, increase gradually over 4-6 weeks, and assess with objective blood tests at 3 months.
")
")




")