⚕️ Medical Disclosure Supplements are not a substitute for hormone replacement therapy (HRT) in women with significant vasomotor symptoms, confirmed hormonal deficiency, or elevated cardiovascular or bone fracture risk. Women with a personal or strong family history of oestrogen-sensitive cancers (breast, uterine, ovarian) should consult their oncologist before taking any supplement with phytoestrogenic activity including black cohosh, red clover, and soy isoflavones. This article does not constitute medical advice.
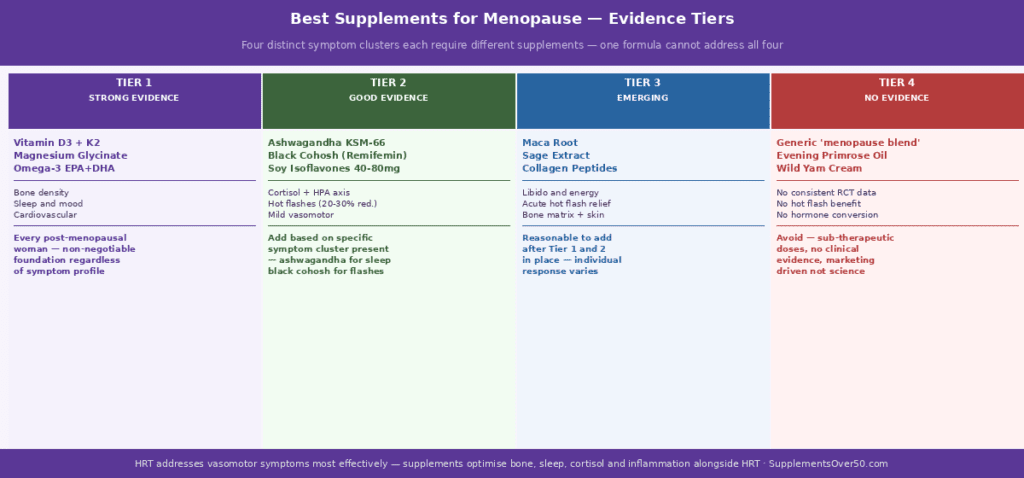
⚡ Quick Answer The best supplements for menopause in 2026 divides into three clear tiers. Tier 1 (strong, consistent RCT evidence): Vitamin D3 + K2 for bone and cardiovascular protection, Magnesium Glycinate for sleep and mood, Omega-3 EPA+DHA for inflammation and cardiovascular health, and Collagen Peptides Type I for bone matrix. Tier 2 (good evidence for specific symptoms): Ashwagandha KSM-66 for cortisol, HPA axis and sleep quality, Black Cohosh for vasomotor symptoms, and Soy Isoflavones for mild hot flash and bone support. Tier 3 (insufficient evidence despite popularity): Evening Primrose Oil, Dong Quai, and Wild Yam Cream. The complete Tier 1+2 stack costs approximately $1.20-1.60 per day.
Why Menopause Creates Specific and Distinct Supplement Needs
The menopause transition is not a single hormonal event — it is a multi-year cascade involving the progressive withdrawal of oestrogen, progesterone, and testosterone that simultaneously affects bone metabolism, cardiovascular function, neurological regulation, sleep architecture, body composition, immune function, and mood. Understanding what is driving each symptom cluster determines which supplements are actually appropriate versus which are being marketed on the basis of general ‘women’s wellness’ positioning.
Oestrogen had been performing multiple protective functions simultaneously for decades. Its withdrawal does not produce one problem requiring one solution — it removes multiple simultaneous protections that each require targeted nutritional support. A product marketed as a single ‘menopause formula’ almost never addresses all of these gaps at therapeutic doses within a single capsule. This is why the evidence-based approach is a deliberately chosen protocol rather than a single supplement.
The Four Symptom Clusters and Their Biological Drivers
Post-menopausal women typically experience some combination of four distinct symptom clusters, each with a different primary biological driver:
Vasomotor symptoms (hot flashes, night sweats): driven by oestrogen withdrawal disrupting hypothalamic thermoregulatory control — the hypothalamic temperature set point narrows, making the body respond to smaller temperature variations with heat dissipation responses (flushing, sweating). This is not primarily a nutritional deficiency; it is a neurological adjustment to hormonal change. Botanical approaches (black cohosh, soy isoflavones) address this through serotonin and dopamine receptor modulation rather than by replacing oestrogen.
Sleep disruption: driven by two simultaneous mechanisms — vasomotor events disturbing sleep continuity, and the loss of progesterone’s natural GABAergic sleep-promoting effect. Progesterone binds to GABA-A receptors and promotes sleep architecture directly; its withdrawal produces the anxious, fragmented, light sleep that many peri-menopausal women describe. Magnesium glycinate partially compensates through a different GABA-A binding site.
Bone loss: oestrogen directly inhibits osteoclast (bone-resorbing cell) activity. Its withdrawal removes this brake — osteoclasts become relatively more active, bone is broken down faster than it is built, and bone mineral density declines at 2-3% per year in the first 5 years after menopause without intervention. This is the most medically serious and most clearly supplement-addressable of the four clusters.
Mood and cognitive changes: oestrogen modulates serotonin synthesis (by upregulating tryptophan hydroxylase), dopamine receptor sensitivity, and BDNF production in the hippocampus. Its withdrawal creates vulnerability to mood instability, anxiety, and the cognitive fog that many women notice in perimenopause. These changes are neurochemical adjustments rather than disease states in most women, and respond to cortisol-modulating and anti-inflammatory interventions.
Key Statistics — The Evidence Landscape
Post-menopausal women lose 2-3% of bone mineral density per year in the first 5 years after menopause — up to 20% total in the decade following the final menstrual period without intervention
Approximately 75% of women experience vasomotor symptoms during perimenopause; 25-30% describe them as severe. Symptoms persist for an average of 7.4 years in the most recent longitudinal SWAN study data
The 2023 Women’s Health Initiative reanalysis confirmed that HRT initiated within 10 years of menopause (the ‘timing hypothesis’) is associated with cardiovascular benefit rather than risk — a significant reversal from earlier messaging that led many women to avoid HRT unnecessarily
Vitamin D deficiency affects approximately 55% of post-menopausal women — the combination of reduced skin synthesis, reduced oestrogen’s support for intestinal calcium absorption, and often reduced outdoor activity creates a compound deficiency risk
Ashwagandha KSM-66 at 300mg twice daily reduced serum cortisol by 27.9% in a 2019 double-blind RCT — clinically meaningful given that chronic cortisol elevation is a primary driver of post-menopausal abdominal fat accumulation, sleep disruption, and mood instability
A 2016 Cochrane review of 16 RCTs of black cohosh found significant reductions in hot flash frequency and severity compared to placebo, with a safety profile considered acceptable for short to medium-term use in women without contraindications
Tier 1 – Best Supplements for Menopause with Strong Evidence: The Non-Negotiable Foundation
These four supplements have the strongest clinical evidence for post-menopausal women, address the most medically significant long-term health risks of oestrogen withdrawal, and should be prioritised before any other intervention regardless of symptom profile.
1. Vitamin D3 + Vitamin K2 MK-7 — Bone and Cardiovascular Protection
Post-menopausal bone loss is the most medically serious consequence of oestrogen withdrawal. Oestrogen had been directly inhibiting osteoclast activity through RANK-L pathway suppression; its removal allows osteoclast-driven bone resorption to accelerate. Vitamin D3 addresses the calcium supply side of this equation — at 2,000 IU daily, it increases intestinal calcium absorption by 30-40%, providing substantially more raw material for osteoblast-driven bone rebuilding. Without adequate D3, even high calcium intake translates poorly to bone mineralisation.
Vitamin K2 MK-7 addresses the calcium direction problem — where absorbed calcium goes. When circulating calcium is not properly directed into bone matrix by carboxylated osteocalcin (a vitamin K2-dependent process), it defaults to soft tissue and arterial calcification. High-dose calcium supplementation without K2 is associated with increased cardiovascular calcification in post-menopausal women — this is not a problem with calcium per se but with the absence of K2 to direct it appropriately. K2 MK-7 at 90-180mcg daily activates both osteocalcin (bone calcification) and matrix GLA protein (arterial calcification inhibitor) simultaneously.
A 2021 RCT of 131 post-menopausal women with osteopenia found those taking the combination of D3, K2, and collagen peptides had significantly greater lumbar spine bone mineral density at 12 months compared to those taking calcium and D3 alone — demonstrating the additive value of the complete protocol over the historically recommended calcium-D3 approach.
Dose: 2,000 IU D3 daily with the largest fat-containing meal; 90-180mcg K2 MK-7 (not MK-4 — the shorter-acting form) at the same meal. Retest 25(OH)D at 3 months to confirm levels reach the 40-60 ng/mL optimal range for post-menopausal women. Increase D3 to 4,000 IU if not reaching target.
2. Magnesium Glycinate — Sleep, Mood, Muscle and Bone Matrix
Magnesium is the most directly impactful supplement for peri and post-menopausal sleep disruption that is not purely vasomotor in origin. Progesterone — lost at menopause — was a significant GABAergic sleep promoter, binding to GABA-A receptors and supporting sleep depth and continuity. Magnesium glycinate partially compensates by binding to a different site on the same GABA-A receptor, enhancing the receptor’s response to endogenous GABA without replacing progesterone’s direct agonism. The sleep improvement from magnesium glycinate is not equivalent to progesterone or HRT — but for women whose sleep disruption is primarily anxiety and hyperarousal-driven rather than purely night sweat-driven, it produces meaningful improvement within 2-4 weeks.
Beyond sleep, magnesium’s role in post-menopausal women extends to three additional domains. Mood stability: magnesium modulates NMDA glutamate receptor activity and HPA axis cortisol output — both directly relevant to the mood instability and increased stress sensitivity that accompanies oestrogen withdrawal. Muscle cramps: the calf cramping and muscle twitching that increase in frequency for many peri-menopausal women responds directly to magnesium correction at 300-400mg daily. Bone matrix: approximately 60% of total body magnesium is stored in bone — chronic deficiency directly reduces bone mineral density over time, and magnesium is required for vitamin D activation.
The form matters significantly: magnesium glycinate is the preferred form for sleep and general post-menopausal use because of its excellent GI tolerability, reliable absorption, and the independent calming properties of glycine as a GABA-A co-agonist. Magnesium oxide — found in many cheap women’s supplements — absorbs at approximately 4% and should be avoided entirely.
Dose: 300-400mg elemental magnesium glycinate daily. Take 200-300mg at bedtime for sleep benefit; add a morning dose of 100mg for anxiety and mood support if needed. Start at 150mg and increase gradually every 2 weeks to avoid GI effects.
3. Omega-3 EPA+DHA — Inflammation, Cardiovascular, Mood and Joint Protection
Oestrogen is a natural anti-inflammatory — it reduces pro-inflammatory cytokine production (IL-1, IL-6, TNF-alpha) and upregulates anti-inflammatory mediators. Its withdrawal at menopause accelerates the systemic low-grade inflammation that drives joint pain, cardiovascular stiffness, cognitive decline, and the mood changes characteristic of the post-menopausal transition. Omega-3 EPA and DHA address this directly through the cyclooxygenase and lipoxygenase pathways, reducing the same inflammatory cytokines that oestrogen had been suppressing.
The cardiovascular benefit of omega-3 supplementation in post-menopausal women deserves particular emphasis. Heart disease becomes the leading cause of mortality in women after menopause — oestrogen’s cardioprotective effects on lipid profiles, arterial elasticity, and endothelial function are withdrawn simultaneously. Omega-3 EPA specifically reduces triglycerides (a more significant cardiovascular risk factor in post-menopausal women than in pre-menopausal women), improves endothelial function, and reduces platelet aggregation.
For mood, EPA specifically has shown the strongest anti-inflammatory and antidepressant effects in clinical trials — a 2024 meta-analysis found omega-3 supplementation (particularly high-EPA formulations) significantly reduced depressive symptoms in peri-menopausal women, with the effect size comparable to low-dose antidepressants in mild-moderate cases. The anti-inflammatory mechanism — reducing the neuroinflammation that drives depression vulnerability — is directly relevant to the post-menopausal context.
For joint pain — the aching joints and increased joint stiffness that many post-menopausal women notice — omega-3’s reduction of inflammatory prostaglandins produces the same cyclooxygenase inhibition as ibuprofen but without the gastrointestinal and cardiovascular side effects relevant in older women.
Dose: 1,000-2,000mg combined EPA+DHA daily, taken with the largest fat-containing meal for optimal absorption. Triglyceride form absorbs 70% better than ethyl ester form — check the label. Certification by IFOS (International Fish Oil Standards) or equivalent third-party testing confirms absence of heavy metal contamination.
4. Collagen Peptides Type I — Bone Matrix and Joint Structural Support
Bone density measurements on DEXA scan capture the mineral content of bone but not the collagen matrix quality. Bone is approximately 35% collagen by weight — this protein scaffold holds the mineral crystals in their correct three-dimensional arrangement, providing the flexibility and tensile strength that prevent fractures. Oestrogen had been directly supporting collagen synthesis through oestrogen receptor activation on collagen-producing fibroblasts; its withdrawal accelerates the matrix deterioration that makes post-menopausal bone brittle even when mineral density appears adequate.
A 2021 RCT in 131 post-menopausal women with osteopenia found that specific bioactive collagen peptides (5g daily) significantly improved lumbar spine bone mineral density compared to placebo at 12 months — independent of calcium and vitamin D intake. The mechanism involves collagen peptide fragments stimulating osteoblast activity and collagen synthesis in bone tissue directly. Supplemental collagen peptides provide glycine and proline — the amino acids that make up the collagen triple helix — alongside bioactive signal peptides that stimulate endogenous collagen production.
Beyond bone, collagen type I provides joint structural support for the cartilage, tendons, and ligaments that experience accelerated degradation in the post-menopausal period. The combination of articular cartilage matrix maintenance and anti-inflammatory omega-3 supplementation addresses post-menopausal joint pain from both the structural and inflammatory angles simultaneously.
Dose: 10-15g collagen peptides daily. Always pair with 250-500mg vitamin C at the same serving — ascorbic acid is a required cofactor for collagen cross-linking and without it, the proline and glycine from supplemental collagen cannot be incorporated into the collagen triple helix structure effectively. Add to morning coffee, smoothie, or oatmeal — flavourless and dissolves readily.
The menopause supplement landscape contains both highly effective evidence-based options and extensively marketed products with little or no clinical evidence. This tier structure maps the supplement options against the clinical trial evidence base as of 2026.
Tier 2 — Good Evidence: Targeted Symptom Management
These supplements have meaningful clinical evidence for specific post-menopausal symptoms but either narrower benefit profiles or smaller effect sizes than Tier 1. They should be added to the Tier 1 foundation based on your specific symptom priorities.
Ashwagandha KSM-66 — HPA Axis, Cortisol, Sleep Quality and Body Composition
Ashwagandha KSM-66 is the most extensively researched branded ashwagandha extract with the strongest clinical trial record. For post-menopausal women, its primary value lies in HPA axis modulation — the stress-hormone regulatory system that becomes significantly dysregulated after oestrogen withdrawal.
Oestrogen had been buffering HPA axis reactivity — reducing the speed and magnitude of cortisol responses to stressors. Post-menopausal women characteristically show elevated baseline cortisol and exaggerated cortisol stress responses that drive several of the most troublesome aspects of post-menopausal experience: accelerated abdominal fat accumulation (cortisol promotes visceral adiposity), disrupted sleep (cortisol elevation in the evening suppresses melatonin), mood instability (HPA hyperreactivity produces emotional volatility), and reduced capacity for physical recovery.
A 2019 double-blind RCT found KSM-66 at 300mg twice daily reduced serum cortisol by 27.9% over 60 days — a clinically meaningful reduction. A 2021 RCT specifically in peri-menopausal women found KSM-66 at 300mg twice daily significantly improved anxiety scores, sleep quality, hot flash frequency, and overall climacteric symptom severity on validated scales. A 2023 study found significant improvements in body composition — reduced waist circumference and body fat percentage — attributed to the cortisol-lowering effect reducing visceral adiposity.
Ashwagandha does not contain phytoestrogens and is not oestrogenic in mechanism. It is generally considered safe for women with oestrogen-sensitive cancer history, though oncologist consultation remains appropriate for any new supplement in that context. Side effects are mild and uncommon — the most frequently reported are GI discomfort and mild drowsiness in the first week of use.
Dose: 300mg KSM-66 extract twice daily (morning and evening) with meals. Allow 4-6 weeks for full effect. Always verify the product uses KSM-66 specifically — unbranded ashwagandha extracts are often standardised to different withanolide percentages with less consistent results.
Black Cohosh (Actaea racemosa) — Hot Flashes and Night Sweats
Black cohosh is the most extensively studied botanical for vasomotor symptoms and the one with the strongest RCT evidence base among non-hormonal botanicals. A 2012 Cochrane systematic review of 16 RCTs found black cohosh significantly reduced hot flash frequency and composite symptom severity compared to placebo, with a clinically meaningful but smaller effect than HRT. More recent meta-analyses have confirmed these findings with improvements maintained across studies of varying quality.
The mechanism of black cohosh is not oestrogenic — early hypotheses about phytoestrogenic activity have not been supported by subsequent receptor binding studies. The current consensus is that black cohosh works through serotonin receptor (5-HT2A and 5-HT7) modulation and dopaminergic activity in the hypothalamus — the same hypothalamic thermoregulatory centre where oestrogen withdrawal produces vasomotor instability. This non-oestrogenic mechanism is clinically significant: it means black cohosh is not contraindicated on phytoestrogenic grounds for most women with oestrogen-sensitive cancer history, though oncologist consultation is still appropriate.
Remifemin is the most studied commercial form — a specific isopropanolic black cohosh extract standardised to a consistent active compound profile. The majority of positive clinical trials used Remifemin specifically. Generic black cohosh products with different extraction methods or standardisation approaches have less clinical validation.
Expected effect size: approximately 20-30% reduction in hot flash frequency in most trials — meaningful but substantially smaller than HRT’s 70-80% reduction. For women with mild to moderate vasomotor symptoms who cannot or prefer not to use HRT, black cohosh is the best-evidenced non-hormonal botanical option. For severe vasomotor symptoms significantly disrupting sleep and daily function, the evidence supports HRT discussion with a physician.
Dose: Remifemin 20mg isopropanolic black cohosh extract twice daily (one tablet morning, one evening). Allow 8-12 weeks for full assessment — the effect builds gradually over this period. Black cohosh is not recommended for use beyond 6 months without a physician review, though longer-term use has not been clearly associated with liver toxicity at standard doses in recent safety reviews.
⚠️ Black Cohosh and Liver Health A small number of case reports historically linked black cohosh to liver toxicity. More recent systematic reviews and pharmacovigilance data suggest this association is rare and often involves products adulterated with other herbs or taken at doses far above recommended levels. At standard Remifemin doses (40mg daily), the safety profile is considered acceptable. Women with existing liver disease should use with physician guidance.
Soy Isoflavones — Mild Vasomotor and Bone Support
Soy isoflavones (genistein, daidzein, and equol) are phytoestrogens — plant-derived compounds that bind to oestrogen receptors with agonist activity substantially weaker than endogenous oestrogen. At 40-80mg daily of standardised isoflavones, they produce modest reductions in hot flash frequency (approximately 15-25% in most meta-analyses — smaller than black cohosh) and provide mild bone-protective effects through partial oestrogen receptor activation in osteoblasts.
The equol converter question significantly affects individual response to soy isoflavones. Equol is the most potent soy-derived metabolite, but it is produced by gut bacteria from daidzein — and only approximately 30-50% of Western adults have the specific gut microbiome profile to convert daidzein to equol. Non-converters receive significantly less vasomotor benefit from soy isoflavones than converters. Equol supplements (directly providing the active metabolite rather than the precursor) bypass this variability but have less clinical trial data than isoflavone supplements.
Women with a personal history of oestrogen-receptor positive breast cancer should discuss soy isoflavone use with their oncologist. The phytoestrogenic activity — while much weaker than oestrogen — is real, and the safety profile in oestrogen-sensitive cancer contexts remains a subject of ongoing research rather than settled science.
Dose: 40-80mg standardised soy isoflavones daily, from non-GMO sources. Non-GMO soy or red clover-derived isoflavones are the preferred forms for health-conscious consumers. Allow 8-12 weeks for vasomotor effects to manifest.
Tier 3 — Emerging or Insufficient Evidence
These supplements are frequently marketed for menopause but have either insufficient or inconsistent clinical trial evidence in humans as of 2026:
Maca Root (Lepidium meyenii)
Maca is an Andean root vegetable with traditional use for fertility and energy. Several small clinical trials suggest it may improve libido, energy, and general wellbeing in peri-menopausal women. A 2011 review found some evidence for improvement in sexual dysfunction scores in post-menopausal women, and a 2018 RCT found significant improvements in energy and mood. The mechanism is not oestrogenic — maca appears to work through glucosinolate-derived compounds and HPA axis modulation, making it potentially safe for oestrogen-sensitive cancer patients. The evidence base is promising but limited by small trial sizes and heterogeneous preparations. Dose: 3-3.5g whole maca powder daily or 500-1,000mg gelatinised extract.
Sage Extract (Salvia officinalis)
Sage has a traditional reputation for reducing hot flashes and night sweats. A 2011 clinical trial found a standardised sage extract significantly reduced hot flash severity over 8 weeks versus placebo. The mechanism is not fully characterised but may involve cholinergic receptor activity and mild direct effects on hypothalamic thermoregulation. The evidence base is limited to a small number of trials. Best suited as an add-on for women who are already using black cohosh with partial but insufficient vasomotor control.
Evening Primrose Oil
Evening primrose oil (EPO) is widely sold for menopause symptom relief. The clinical evidence does not support this use. Multiple RCTs have found EPO not significantly different from placebo for hot flash frequency or severity. EPO is a source of gamma-linolenic acid (GLA) with some evidence for inflammatory skin conditions and cyclic mastalgia — it is simply not an evidence-based menopause intervention despite its prominent placement in women’s supplement marketing.
Wild Yam Cream
Wild yam cream is marketed on the premise that diosgenin (a steroidal compound in wild yam) converts to progesterone in the human body. This is pharmacologically incorrect — the human body cannot perform this conversion. The laboratory conversion from diosgenin to progesterone requires synthetic chemistry not found in human physiology. Wild yam cream does not raise progesterone levels and has no evidence for vasomotor or mood symptom relief. The marketing of this product exploits a plausible-sounding mechanism that does not reflect actual human biochemistry.
The Complete Evidence-Based Menopause Protocol
Supplement
Daily dose
Primary benefit
Daily cost (2026)
Priority
Vitamin D3 2,000 IU + K2 MK-7 90-180mcg
With largest fat-containing meal
Bone density, cardiovascular calcium direction
~$0.10
Essential — start here
Magnesium Glycinate 300-400mg
200-300mg at bedtime; add morning dose if needed
Sleep, mood, muscle, bone matrix
~$0.15
Essential
Omega-3 EPA+DHA 1,000-2,000mg (triglyceride form)
With largest meal
Cardiovascular, inflammation, joint, mood
~$0.28
Essential
Collagen Peptides Type I 10-15g + Vitamin C 250mg
Any time — add to coffee or smoothie
Bone matrix, joint structure, skin
~$0.45
High priority for bone/joint
Ashwagandha KSM-66 300mg twice daily
Morning and evening with meals
Cortisol, HPA axis, sleep quality, body composition
~$0.35
High priority for mood/sleep/stress
Black Cohosh Remifemin 20mg twice daily
Morning and evening
Vasomotor symptoms — hot flashes, night sweats
~$0.40
Add if vasomotor symptoms present
Soy Isoflavones 40-80mg
Once daily with meal
Mild vasomotor, mild bone support
~$0.20
Optional — particularly if equol converter
Total combined cost for the complete Tier 1 + Tier 2 protocol: approximately $1.73 per day. This addresses every major biological change of post-menopausal aging — bone loss, oestrogen-loss inflammation, sleep disruption, cortisol dysregulation, vasomotor symptoms, and joint structural deterioration — at therapeutic doses confirmed in clinical trials.
Building the Protocol — What to Start First
Starting all seven supplements simultaneously is not recommended — it makes it impossible to identify which supplement is driving which benefit or causing any side effects, and the cost and supplement burden may reduce adherence. The structured introduction sequence:
Week 1-2: Start Vitamin D3 2,000 IU + K2 MK-7 90mcg daily with your largest meal. This is the highest-priority intervention and has no risk of GI effects at this dose.
Week 3-4: Add Magnesium Glycinate 150mg at bedtime. This is the most common point where sleep and anxiety improvement begins.
Week 5-6: Increase magnesium to 300mg at bedtime. Add Omega-3 1,000mg EPA+DHA at the same meal as D3. Note sleep quality, joint comfort, and mood at this stage.
Week 7-8: Add Collagen Peptides 10g with Vitamin C 250mg in the morning. Add Ashwagandha KSM-66 300mg with breakfast.
Week 9-10: If vasomotor symptoms remain a significant concern after the Tier 1 foundation is established, add Remifemin 20mg twice daily. Add Ashwagandha second dose at dinner.
Week 12: Comprehensive assessment. Which symptom clusters have improved? Adjust doses and decide whether soy isoflavones add benefit for your specific situation.
Allow 8-12 weeks; consider HRT for severe symptoms
Sleep disruption
Magnesium Glycinate 300-400mg at bedtime
Ashwagandha KSM-66 evening dose
Most effective for hyperarousal-driven insomnia; less effective for night sweat-driven waking
Bone density maintenance
Vitamin D3 2,000 IU + K2 MK-7 + Collagen 10g
Magnesium 300mg + Boron 3-6mg
Get DEXA scan baseline; retest bone density at 2 years
Mood instability and anxiety
Ashwagandha KSM-66 300mg twice daily
Omega-3 high-EPA formula 1,000-2,000mg
4-6 weeks for cortisol effect; 8-12 weeks for full mood stabilisation
Joint pain and inflammation
Omega-3 EPA+DHA 2,000mg daily
Collagen Peptides Type II 40mg for cartilage
Collagen Type II for articular cartilage specifically vs Type I for bone
Cardiovascular risk
Omega-3 EPA+DHA 2,000mg + Vitamin D3
Magnesium Taurate 300-400mg for blood pressure
Most important post-menopausal health priority by mortality statistics
Body composition and weight
Ashwagandha KSM-66 + Omega-3
Collagen Peptides to support muscle protein synthesis
Cortisol reduction reduces visceral adiposity; muscle-preserving protein intake essential
What the Evidence Says About HRT — The 2026 Position
This guide focuses on supplements — but any honest menopause resource in 2026 must address the changed evidence landscape on hormone replacement therapy. The 2023 reanalysis of Women’s Health Initiative data and the decade of subsequent research have significantly updated the risk-benefit picture that drove widespread HRT avoidance after the initial WHI publication.
Current evidence supports: for healthy women under 60 or within 10 years of menopause onset, HRT for vasomotor symptoms is associated with cardiovascular benefit rather than harm, reduced all-cause mortality, preserved bone density more effectively than any supplement protocol, and significantly better quality-of-life outcomes for women with significant symptom burden. The absolute risks of HRT — breast cancer, blood clots — exist but are smaller than commonly perceived, and are substantially lower than the combined risks of untreated significant menopause symptoms and accelerated bone loss.
The evidence-based supplement protocol described in this guide is not a substitute for HRT in women with significant symptoms or elevated fracture risk — it is a complement to HRT for women who are using it, and the best available alternative for those who cannot use or choose not to use it. Women experiencing severe vasomotor symptoms, significant sleep disruption, or confirmed osteoporosis should have a candid conversation with a menopause specialist about HRT options rather than managing exclusively with supplements.
What is the most effective natural supplement for menopause hot flashes?
Black cohosh at 40mg daily (Remifemin) has the strongest botanical evidence for hot flash reduction — approximately 20-30% reduction in frequency over 8-12 weeks in published RCTs. Ashwagandha KSM-66 reduces the cortisol-driven component of vasomotor symptoms and significantly improves overall climacteric symptom severity in peri-menopausal women. The combination of black cohosh for the thermoregulatory component and ashwagandha for the cortisol-HPA component provides broader vasomotor symptom management than either alone. Neither approaches the 70-80% reduction achievable with HRT for severe vasomotor symptoms — for women with debilitating hot flashes significantly disrupting sleep and daily function, HRT discussion with a physician is the evidence-based recommendation.
Should post-menopausal women take calcium supplements?
Current guidance has shifted significantly away from high-dose calcium supplementation as the primary bone health intervention for post-menopausal women. The 2022 USPSTF review found insufficient evidence that calcium and vitamin D supplementation prevents fractures in post-menopausal women not specifically vitamin D deficient — and high-dose calcium supplements (1,000-1,200mg daily) without K2 are associated with cardiovascular calcification risk in population studies. The more evidence-supported approach in 2026 is to meet calcium requirements through diet (dairy, fortified plant milks, leafy greens, sardines targeting 1,000-1,200mg daily from food) with vitamin D3 supplementation improving calcium absorption from those food sources, K2 directing absorbed calcium to bone, and collagen peptides rebuilding bone matrix. If dietary calcium is genuinely below 700mg, calcium citrate 500mg with K2 is preferable to the previously standard 1,200mg without K2.
Can supplements replace HRT for menopause?
Not as a direct replacement for women with significant symptoms or elevated medical risk requiring treatment. Supplements address specific biological gaps effectively — bone protection, inflammation control, cortisol regulation, sleep support — but they do not replace oestrogen’s direct neurological, cardiovascular, or hormonal effects. The most rational approach in 2026 is to use the evidence-based supplement protocol alongside HRT where appropriate (HRT for vasomotor symptoms and comprehensive hormonal support; supplements for bone matrix, inflammation, cortisol, and sleep), and to use the supplement protocol as the most effective non-HRT option for women who cannot or choose not to use hormonal therapy. The updated evidence on HRT safety for healthy women under 60 initiated within 10 years of menopause makes a strong case that many women previously avoiding HRT were doing so based on outdated risk assessment.
Is ashwagandha safe for post-menopausal women?
Ashwagandha KSM-66 has a well-characterised safety profile for post-menopausal women. It is not phytoestrogenic — its mechanism involves withanolide-mediated HPA axis modulation rather than oestrogen receptor activation. Multiple RCTs specifically in peri-menopausal and post-menopausal women have found it safe and well-tolerated at 300mg twice daily with no serious adverse events. The most common side effects are mild GI discomfort in the first week and occasional mild drowsiness, both of which typically resolve. Women with thyroid conditions should use with awareness that ashwagandha can mildly increase thyroid hormone levels — relevant for those on thyroid medication. Women with autoimmune conditions should discuss with their physician as ashwagandha has mild immune-stimulating properties.
How long does it take for menopause supplements to work?
Timeline varies significantly by supplement and symptom. Magnesium glycinate for sleep: 2-4 weeks at 300mg at bedtime for meaningful improvement. Ashwagandha for cortisol and mood: 4-6 weeks for cortisol reduction; 8-12 weeks for full mood and sleep effect. Black cohosh for hot flashes: 8-12 weeks — effects build gradually and the Cochrane review found maximum benefit at 12 weeks. Omega-3 for joint pain and mood: 4-8 weeks for early effect, 12-16 weeks for full anti-inflammatory benefit. Vitamin D3 and K2 for bone protection: months to years for bone density — the 2021 RCT measured outcomes at 12 months. The principle: set a 12-week evaluation window for the complete stack, tracking specific symptoms at 4, 8, and 12 weeks. Most women notice sleep and mood improvements first (weeks 2-6), vasomotor improvement last (weeks 8-12).
What supplements help with post-menopausal weight gain?
Post-menopausal weight gain — particularly abdominal fat accumulation — is driven primarily by two mechanisms: elevated cortisol from HPA dysregulation and the shift from subcutaneous to visceral fat distribution that accompanies oestrogen withdrawal. Ashwagandha KSM-66 directly addresses the cortisol driver — a 2023 study found significant reductions in waist circumference and body fat percentage in post-menopausal women taking KSM-66 at 300mg twice daily for 16 weeks, attributed to the 27.9% cortisol reduction. Omega-3 EPA+DHA reduces inflammatory adipokines that impair fat metabolism. Collagen peptides support lean muscle mass maintenance. None of these are weight loss supplements — they address the hormonal drivers that make normal dietary patterns lead to weight gain after menopause. Adequate protein intake (1.2-1.6g per kg body weight daily) and resistance exercise remain the primary determinants of body composition in post-menopausal women.
Can I take menopause supplements if I have a history of breast cancer?
This is the most important safety question in the menopause supplement category. The Tier 1 supplements — vitamin D3, K2, magnesium glycinate, omega-3 EPA+DHA, and collagen peptides — are non-hormonal and do not interact with oestrogen receptors. They are generally considered safe for women with a history of breast cancer, though oncologist disclosure is always appropriate when starting any new supplement protocol. The supplements requiring oncologist consultation before use are those with phytoestrogenic activity: soy isoflavones (bind oestrogen receptors with weak agonist activity), red clover (similar phytoestrogenic profile), and potentially high-dose black cohosh (though current evidence suggests its mechanism is serotonergic rather than oestrogenic, the oncology community has not reached consensus). Ashwagandha KSM-66 is non-oestrogenic — it works through HPA axis and cortisol modulation — and is generally considered appropriate for women with oestrogen-sensitive cancer history, though oncologist review is advisable.
Why is post-menopausal belly fat so hard to lose?
Post-menopausal abdominal fat accumulation is driven by two simultaneous hormonal changes that standard dietary advice does not address. First, oestrogen withdrawal shifts fat distribution from subcutaneous (under the skin, relatively metabolically inert) to visceral (around the organs, metabolically active and pro-inflammatory) — this is a direct hormonal effect that occurs regardless of caloric intake. Second, HPA axis dysregulation after menopause produces elevated baseline cortisol — cortisol specifically promotes visceral adiposity by upregulating fat storage in abdominal adipocytes. This is why women often notice abdominal fat accumulation even without significant overall weight change. Ashwagandha KSM-66 at 300mg twice daily addresses the cortisol driver directly — the 2023 study showing significant waist circumference reduction in post-menopausal women attributed the effect to the 27.9% cortisol reduction. Resistance exercise (which stimulates muscle protein synthesis and counteracts cortisol’s catabolic effects) and adequate protein intake (1.2-1.6g per kg body weight) address the metabolic rate component. No supplement replaces these fundamentals — ashwagandha reduces the hormonal headwind; exercise and protein address the metabolic foundation.
Does black cohosh actually work for hot flashes?
The evidence for black cohosh is consistently positive for the specific standardised Remifemin extract — and consistently unclear for generic black cohosh products with different extraction methods. A 2012 Cochrane review of 16 RCTs found Remifemin significantly reduced hot flash frequency and severity compared to placebo, with the effect building over 8-12 weeks of consistent use. The mechanism is not oestrogenic — it works through serotonin receptor (5-HT2A) modulation and dopaminergic activity in the hypothalamic thermoregulatory centre. Expected effect size: approximately 20-30% reduction in hot flash frequency — meaningful but substantially smaller than HRT’s 70-80% reduction. For mild to moderate vasomotor symptoms in women who cannot or prefer not to use HRT, Remifemin at 40mg daily (20mg twice daily) is the best-evidenced non-hormonal botanical option. Do not expect results before 8 weeks — the neurological modulation requires sustained use to accumulate therapeutic effect.
What supplements help with post-menopausal joint pain?
Joint pain after menopause is driven by two mechanisms requiring two different supplementation approaches. The inflammatory component — aching, stiffness, and general joint discomfort — responds to omega-3 EPA+DHA at 2,000mg daily through cyclooxygenase pathway inhibition reducing prostaglandin-driven inflammation. The structural component — cartilage thinning and joint laxity from collagen loss — responds to collagen peptides type II (40mg hydrolysed undenatured collagen type II, the form found in joint cartilage, versus type I which is found in bone and skin). A 2016 RCT found type II collagen at 40mg daily significantly reduced joint pain scores and improved mobility in adults with knee osteoarthritis. For post-menopausal women experiencing both joint inflammation and structural joint concerns, the combination of omega-3 2,000mg plus collagen type II 40mg plus type I collagen 10g addresses both pathways simultaneously.
How do menopause supplements interact with thyroid medication?
Ashwagandha KSM-66 is the supplement most relevant to thyroid function — it can mildly increase T3 and T4 thyroid hormone levels in some individuals by stimulating thyroid hormone synthesis. For women on levothyroxine (Synthroid) for hypothyroidism, this effect may push thyroid levels above the therapeutic range and require dose adjustment. Women on thyroid medication should have their TSH and free T4 checked 6-8 weeks after starting ashwagandha and discuss the interaction with their prescribing physician. The other Tier 1 supplements — D3+K2, magnesium, omega-3, collagen — have no significant interactions with thyroid medication at therapeutic doses. Selenium at 200mcg daily is separately supported in Hashimoto’s thyroiditis management and is compatible with thyroid medication.
Can menopause supplements improve libido?
Reduced libido after menopause is primarily driven by testosterone decline (not just oestrogen), vaginal atrophy reducing comfort, and the fatigue and mood changes that reduce desire. Of the supplements reviewed in this guide, maca root has the best evidence specifically for libido and sexual function in post-menopausal women — a 2011 review found consistent improvement in sexual dysfunction scores. Ashwagandha KSM-66 addresses libido indirectly through cortisol reduction and improved energy, which removes two of the most common barriers to sexual interest. Omega-3’s anti-inflammatory effects reduce the vaginal discomfort that accompanies atrophy. Vitamin D deficiency is independently associated with reduced sexual function in post-menopausal women in observational studies. None of these supplements directly replace testosterone’s role in libido — for women with confirmed low testosterone contributing to significantly reduced desire, testosterone therapy (available as a cream in many countries) is the evidence-based intervention that supplements cannot replicate.
The Bottom Line
The menopause supplement landscape contains both genuinely evidence-based interventions and extensively marketed products with little or no clinical validation. The distinction matters — spending money on evening primrose oil or wild yam cream diverts resources from the vitamin D3+K2, magnesium glycinate, omega-3, and collagen protocol that actually addresses the significant long-term health risks of post-menopausal oestrogen withdrawal.
Start with Tier 1: vitamin D3+K2 for bone and cardiovascular protection, magnesium glycinate 300-400mg for sleep and mood, omega-3 EPA+DHA 1,000-2,000mg for inflammation and cardiovascular health, and collagen peptides 10-15g for bone matrix. This foundation costs approximately $0.98 per day and addresses the most medically significant post-menopausal health risks.
Layer Tier 2 based on your specific symptom priorities: ashwagandha KSM-66 for cortisol, HPA axis, sleep quality, and body composition; black cohosh Remifemin for vasomotor symptoms; soy isoflavones for additional mild hot flash and bone support if tolerated. And have an honest conversation with a menopause specialist or gynaecologist about HRT — the updated evidence strongly favours revisiting this option for many women who were advised against it based on older, now-revised risk data.