| ⚕️ Medical Disclosure Severe vitamin B12 deficiency causing neurological symptoms — numbness or tingling in the hands or feet, difficulty walking or balance problems, significant memory impairment, or pronounced cognitive decline — requires physician assessment and potentially intramuscular B12 injections rather than oral supplementation. Vitamin B12 Dosage Seniors includes Oral supplementation corrects mild to moderate deficiency efficiently but may be too slow for neurological recovery in advanced deficiency. Do not delay physician evaluation of neurological symptoms to attempt oral supplementation first. |
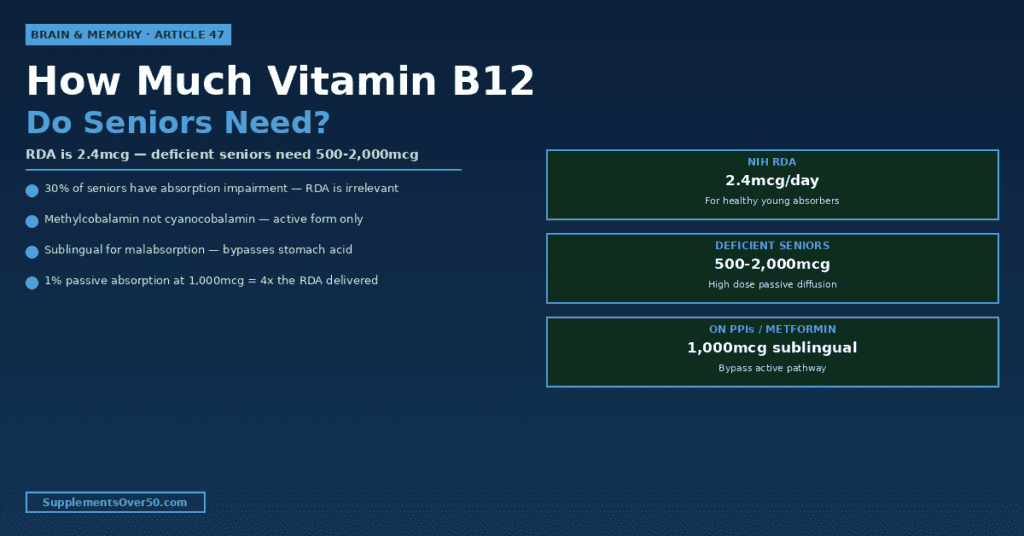
| ⚡ Quick Answer The NIH RDA for vitamin B12 is 2.4mcg daily — designed for young healthy adults with normal stomach acid and intact intrinsic factor production. Up to 30% of adults over 50 have atrophic gastritis that significantly impairs B12 absorption from food, making dietary intake and the RDA essentially irrelevant for them regardless of how much B12 is consumed. For deficiency prevention in healthy seniors over 60 without absorption issues: 25-100mcg methylcobalamin daily. For confirmed mild-moderate deficiency: 500-1,000mcg daily. For seniors on PPIs or with atrophic gastritis: 1,000-2,000mcg daily as sublingual methylcobalamin. Always choose methylcobalamin over cyanocobalamin. The form and the route of administration matter as much as the dose. |
The B12 Paradox — Why the RDA Is Irrelevant for Vitamin B12 Dosage Seniors
Vitamin B12 is unique among essential nutrients in the complexity of its absorption system. Every other water-soluble vitamin absorbs passively across the gut wall with reasonable efficiency. B12 requires an elaborate two-step process involving a specialised protein produced in the stomach — and it is this process, not dietary intake, that fails in a significant proportion of adults over 60.
The NIH RDA of 2.4mcg was derived from absorption studies conducted in young healthy adults with optimal stomach acid production and intact intrinsic factor secretion. These assumptions are valid for most adults under 50. After 60, they increasingly fail — and when they fail, the RDA becomes meaningless as a target because the limiting factor is no longer how much B12 is consumed but how much can actually be absorbed.
This is the B12 paradox that affects millions of seniors: they eat B12-containing foods regularly, they take multivitamins containing the RDA, their physician tells them their diet is adequate — yet they are quietly becoming deficient over months and years because their absorption system is silently failing. Understanding how and why this happens is essential for choosing the right supplemental dose.
For the full picture of what B12 deficiency does to the body after 60: Signs of Vitamin B12 Deficiency in Adults Over 60 — And What to Do
The B12 Absorption System — How It Works and Why It Fails
Step 1 — Stomach Acid Release
Dietary B12 — in meat, fish, eggs, and dairy — is bound tightly to food proteins. Before it can be absorbed, it must be released from these proteins. This release requires stomach acid (hydrochloric acid) to denature the food protein, and pepsin (a gastric enzyme) to cleave the protein-B12 bond. Once released, free B12 binds to haptocorrin (also called R-protein), a glycoprotein secreted in saliva that protects B12 from the acidic stomach environment.
Popular Supplement Guides:
")

")


")
This first step fails partially in the majority of adults over 60. Stomach acid production declines with age — a condition called hypochlorhydria — reducing the efficiency of protein-bound B12 release. Studies show that adults over 60 have on average 20-40% lower gastric acid secretion than young adults. Atrophic gastritis — chronic inflammation causing progressive atrophy of stomach acid-secreting cells — produces a more severe and irreversible form of this impairment, affecting up to 30% of adults over 50. In both conditions, dietary B12 passes through the stomach incompletely released and incompletely absorbed.
Step 2 — Intrinsic Factor Binding
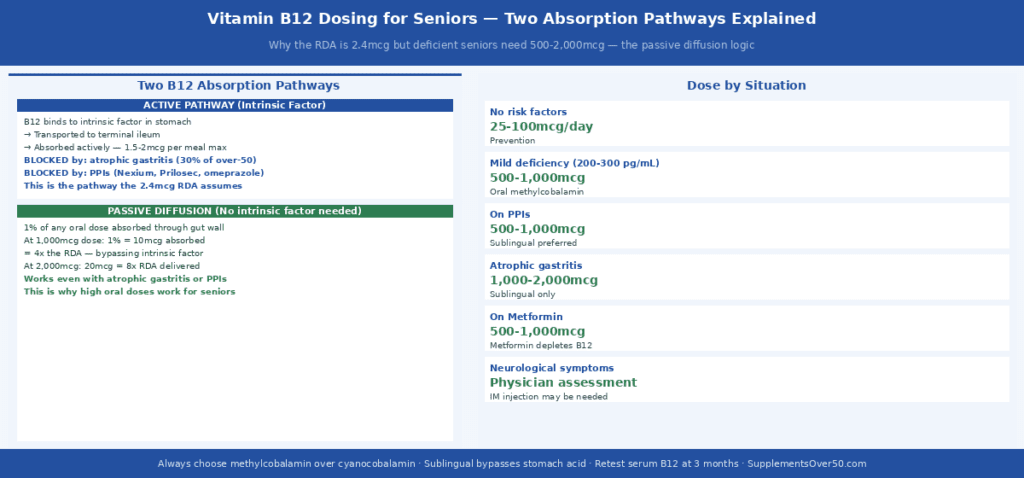
Once free B12 reaches the duodenum, haptocorrin is degraded by pancreatic proteases and B12 transfers to intrinsic factor (IF) — a glycoprotein produced exclusively by parietal cells in the stomach lining. The B12-IF complex is highly stable and protected from intestinal degradation. It travels the length of the small intestine to the terminal ileum, where specific IF receptors (cubilin and amnionless) recognise the complex and transport it across the intestinal wall into the bloodstream.
This intrinsic factor step is where the most clinically significant absorption failures occur in seniors. Atrophic gastritis destroys parietal cells — the same cells that produce both stomach acid and intrinsic factor. As parietal cell mass declines, intrinsic factor production falls proportionally. When IF production drops below the threshold needed to bind all available dietary B12, absorption becomes severely restricted regardless of intake. In complete pernicious anaemia (autoimmune destruction of parietal cells with zero IF production), the active absorption pathway is entirely blocked.
The practical consequence: in a senior with moderate atrophic gastritis, even eating a B12-rich meal of salmon or beef liver does not produce meaningful B12 absorption. Their IF production is insufficient to bind and transport the available B12 to the terminal ileum receptors. This is why ‘my diet is adequate’ is clinically meaningless for seniors with impaired IF production.
The Passive Diffusion Pathway — Why High Doses Work
A second, completely independent B12 absorption pathway exists that does not require intrinsic factor and is not impaired by atrophic gastritis or stomach acid deficiency. This passive diffusion pathway absorbs approximately 1% of any oral B12 dose directly across the intestinal mucosa through non-specific diffusion — no protein binding, no IF, no terminal ileum receptors required.
At the RDA dose of 2.4mcg, passive diffusion contributes negligibly — 1% of 2.4mcg is 0.024mcg, clinically meaningless. But at pharmacological supplement doses, passive diffusion becomes the primary absorption route for deficient seniors: 1% of 1,000mcg is 10mcg — more than four times the RDA delivered through a pathway entirely independent of the failing active absorption system. At 2,000mcg, passive diffusion delivers 20mcg — eight times the RDA.
This is the entire pharmacological logic of high-dose oral B12 supplementation for seniors with impaired absorption: the dose is intentionally high not because seniors need more B12 than younger adults, but because passive diffusion’s fixed 1% efficiency means only a pharmacologically large dose delivers a physiologically adequate amount. The ‘excess’ is not used — it is simply excreted in urine, which is safe for a water-soluble vitamin with no established upper limit.
| ⚡ The Passive Diffusion Calculation At 1,000mcg oral dose: 1% passive diffusion = 10mcg absorbed — 4× the RDA At 2,000mcg oral dose: 1% passive diffusion = 20mcg absorbed — 8× the RDA At the standard multivitamin dose (25mcg): 1% = 0.25mcg — essentially zero for deficient seniors This is why multivitamin B12 doses are completely inadequate for seniors with any absorption impairment |
Key Statistics — The Scope of Senior B12 Deficiency
- Up to 30% of adults over 50 have atrophic gastritis with impaired B12 absorption from food — the most common cause of B12 deficiency in seniors is absorption failure, not inadequate dietary intake
- Approximately 20% of adults over 60 have serum B12 below 200 pg/mL (clinically deficient) and up to 40% have suboptimal levels below 400 pg/mL when functional biomarkers are assessed
- Up to 30% of seniors taking metformin for diabetes have vitamin B12 deficiency — metformin’s blockade of the ileal calcium transporter impairs B12-IF complex absorption directly
- PPIs taken long-term reduce B12 absorption by impairing the stomach acid needed for protein-bound B12 release from food — a 2015 Journal of the American Medical Association study found long-term PPI use associated with a 65% higher B12 deficiency risk
- Neurological damage from B12 deficiency can occur before anaemia develops — the classic teaching that megaloblastic anaemia precedes neurological symptoms is not reliable in folate-supplemented populations
- B12 deficiency is reversible in most cases when identified early — but neurological damage from subacute combined degeneration of the spinal cord may not fully reverse even with aggressive treatment if present for more than 12 months
Why Methylcobalamin Is Always Better Than Cyanocobalamin
The form of B12 in a supplement matters significantly for seniors — and most cheap supplements, multivitamins, and fortified foods use the wrong form. Understanding why requires understanding what happens to different B12 forms after they are absorbed.
Cyanocobalamin — The Cheap and Inadequate Form
Cyanocobalamin is the synthetic form of B12 used in the vast majority of supplements, fortified foods, and standard multivitamins. It is cheap to manufacture, chemically stable, and has been the standard supplementation form for decades. However, cyanocobalamin is not a form that the human body uses directly. After absorption, it must be converted to one of the two active coenzyme forms — methylcobalamin or adenosylcobalamin — before it can participate in cellular metabolism.
This conversion requires the MTHFR (methylenetetrahydrofolate reductase) enzyme pathway. Approximately 30-40% of adults carry genetic variants in the MTHFR gene that reduce enzyme efficiency — meaning that for this substantial proportion of the population, cyanocobalamin conversion to active coenzyme forms is impaired. These individuals may supplement with cyanocobalamin and show normal serum B12 levels while having insufficient active methylcobalamin for neurological and methylation functions.
Additionally, cyanocobalamin contains a cyanide molecule that must be removed and detoxified before conversion can proceed. While the cyanide content is too small to be acutely toxic at supplementation doses, it represents an unnecessary metabolic burden — particularly for heavy smokers (who already have compromised cyanide detoxification) and seniors with reduced detoxification capacity.
Cyanocobalamin has a shorter retention half-life than methylcobalamin — it is excreted more rapidly, requiring more consistent daily supplementation to maintain adequate tissue levels. For seniors who occasionally miss doses, methylcobalamin’s longer tissue retention provides more sustained protection.
Methylcobalamin — The Active, Preferred Form
Methylcobalamin is one of the two active coenzyme forms of B12 that cells use directly. It does not require MTHFR conversion — it is immediately bioavailable to the methylation cycle and neurological B12 functions. For seniors, the neurological advantage is particularly significant: methylcobalamin is the predominant form of B12 in the brain and nervous system, and several studies have found it produces better neurological outcomes than cyanocobalamin in adults with B12 deficiency neuropathy.
A 2020 study found that methylcobalamin specifically — not cyanocobalamin — was associated with improved outcomes in peripheral neuropathy and cognitive function in older adults with B12 deficiency. The nerve regeneration mechanism may be specific to methylcobalamin as the methyl group donor for myelin synthesis and neurotrophic factor production.
Methylcobalamin is also the form most readily available as sublingual (dissolving) tablets, which is clinically important for seniors with malabsorption — sublingual administration bypasses the entire gastric and intrinsic factor-dependent absorption system by absorbing directly through the oral mucosa into the bloodstream.
Adenosylcobalamin — The Mitochondrial Form
Adenosylcobalamin is the second active coenzyme form, functioning primarily in mitochondrial energy metabolism. Some practitioners recommend supplements combining methylcobalamin and adenosylcobalamin (‘dibencozide’) for comprehensive B12 repletion targeting both the methylation cycle and mitochondrial function. For most seniors, methylcobalamin alone at adequate doses is sufficient — adenosylcobalamin combinations are more relevant in specific metabolic conditions.
| Form | Conversion required | MTHFR dependence | Tissue retention | Best use |
| Cyanocobalamin | Yes — to methyl or adenosyl form | Yes — MTHFR variants impair conversion | Lower | Fortified foods only — not recommended for senior supplementation |
| Methylcobalamin | No — active immediately | No — bypasses MTHFR entirely | Higher — stored longer in tissues | All senior B12 supplementation — always preferred |
| Adenosylcobalamin | No — active immediately | No | Higher | Mitochondrial support — combine with methylcobalamin for complete repletion |
| Hydroxocobalamin | Yes — to methyl or adenosyl | Partial — some conversion required | Highest retention | IM injection form — used for severe deficiency treatment |
Sublingual vs Oral Tablets — The Route Matters for Malabsorbers
For seniors with normal stomach acid and normal intrinsic factor production, swallowed oral tablets at high doses (1,000mcg) are perfectly adequate — passive diffusion at 1% of 1,000mcg delivers 10mcg, well above requirements. For seniors with confirmed atrophic gastritis, achlorhydria, or who are on PPIs long-term, sublingual administration is substantially more reliable.
Sublingual B12 dissolves under the tongue and absorbs directly through the oral mucosa — the sublingual veins drain directly into systemic circulation, entirely bypassing the stomach, intrinsic factor requirement, and terminal ileum absorption. This is not passive diffusion — it is direct vascular absorption. A well-formulated sublingual 1,000mcg methylcobalamin tablet absorbs approximately 40-50% of the dose this way, delivering 400-500mcg to the bloodstream — dramatically more than the 10mcg from swallowed passive diffusion.
For the comparison: a senior with atrophic gastritis taking a swallowed 1,000mcg methylcobalamin tablet may absorb 10mcg (passive diffusion only — active pathway blocked). The same senior taking a sublingual 1,000mcg tablet may absorb 400-500mcg (direct oral mucosal absorption). This is a 40-50x difference in absorption at the same dose — making the route of administration far more important than the precise dose for malabsorbing seniors.
Technique for sublingual tablets: place under the tongue, allow to dissolve completely (typically 1-3 minutes depending on the formulation), resist swallowing until fully dissolved. Do not eat or drink for 5-10 minutes after to avoid washing away residual mucosal absorption. Sublingual sprays provide similar benefit through the same mechanism.
| ⚠️ The Multivitamin B12 Problem The most common senior B12 supplementation mistake: relying on a standard multivitamin for B12 coverage. Most multivitamins contain 6-25mcg of cyanocobalamin. For a healthy young adult with intact absorption, this may be adequate. For a senior over 60 with any absorption impairment — the situation that applies to approximately 30-40% of this population — this is completely insufficient on two counts: the wrong form (cyanocobalamin requiring MTHFR conversion) and the wrong dose (6-25mcg provides essentially zero passive diffusion at malabsorbing levels). If your multivitamin is your only B12 source and you are over 60, add a dedicated methylcobalamin supplement at 500-1,000mcg daily. |
Complete Dosing Guide — By Situation
| Situation | Recommended daily dose | Form | Route | Retest at |
| Healthy adult over 60, no risk factors | 25–100mcg daily | Methylcobalamin | Oral tablet | Annually with routine bloodwork |
| Confirmed mild deficiency (serum B12 200-300 pg/mL) | 500–1,000mcg daily | Methylcobalamin | Oral tablet or sublingual | 3 months — confirm levels rising to >400 pg/mL |
| Confirmed moderate deficiency (serum B12 <200 pg/mL) | 1,000–2,000mcg daily | Methylcobalamin | Sublingual preferred | 3 months — may need IM injection if oral inadequate |
| On PPIs (any proton pump inhibitor long-term) | 500–1,000mcg daily | Methylcobalamin | Sublingual — bypasses acid-dependent release | Annually; every 6 months if on PPI >2 years |
| Confirmed atrophic gastritis | 1,000–2,000mcg daily | Methylcobalamin | Sublingual only — active pathway blocked | 3 months; consider IM injection for severe cases |
| On metformin (diabetes medication) | 500–1,000mcg daily | Methylcobalamin | Sublingual preferred | Every 6 months — metformin depletes B12 continuously |
| Vegan or strict plant-based diet | 250–1,000mcg daily | Any B12 form acceptable | Oral | Annually — no dietary B12 source at all |
| Neurological symptoms present | Physician assessment — potentially IM injection | Hydroxocobalamin (IM) | Intramuscular injection | Physician-directed — typically 3 months weekly injections then monthly |
What Your B12 Blood Test Result Means
Serum B12 is the standard test ordered in routine blood panels. Understanding the reference ranges and their limitations is essential for seniors making supplementation decisions:
| Serum B12 level | Classification | Clinical significance | Recommended action |
| Below 150 pg/mL (110 pmol/L) | Severe deficiency | Neurological damage risk — megaloblastic anaemia likely | Urgent physician assessment; IM injection often required |
| 150–200 pg/mL (110-148 pmol/L) | Deficiency | Neurological symptoms probable; fatigue, cognitive impairment | Physician review; 1,000-2,000mcg sublingual methylcobalamin daily |
| 200–300 pg/mL (148-221 pmol/L) | Low — supplementation indicated | Subclinical symptoms common — fatigue, brain fog, memory issues | 500-1,000mcg methylcobalamin daily; retest at 3 months |
| 300–400 pg/mL (221-295 pmol/L) | Suboptimal for seniors | Below functional optimal for adults over 60 — supplement | 100-500mcg methylcobalamin daily to reach >400 pg/mL target |
| 400–700 pg/mL (295-516 pmol/L) | Adequate — optimal range for seniors | Well-supplied — neurological protection likely adequate | Maintain with 25-100mcg daily maintenance dose |
| Above 900 pg/mL (664 pmol/L) | Elevated — investigate cause | Not from supplements alone — consider liver disease, myeloproliferative disorder | Physician review to exclude pathological cause |
An important limitation of serum B12 testing: serum B12 measures total circulating B12 including inactive forms bound to haptocorrin that are not functionally available to cells. Some seniors with apparently normal serum B12 (300-400 pg/mL) have elevated methylmalonic acid (MMA) and homocysteine — functional biomarkers that indicate insufficient active B12 at the cellular level despite adequate circulating levels. If serum B12 appears borderline normal but symptoms persist, request methylmalonic acid testing for a more accurate functional assessment.
For the complete list of B12 deficiency signs that are commonly missed or misattributed to aging — including the peripheral symptoms that appear before blood levels become abnormal — see: Signs of Vitamin B12 Deficiency in Adults Over 60 and What to Do
Medications That Deplete Vitamin B12
Several of the most commonly prescribed medications in adults over 60 actively reduce B12 status — either by impairing absorption or increasing urinary losses. Seniors on these medications should consider themselves at high risk of B12 insufficiency regardless of dietary intake:
| Medication | Depletion mechanism | Estimated prevalence in seniors | Recommended supplemental dose |
| Metformin (Glucophage, Glumetza) | Blocks ileal calcium-dependent transporter — directly impairs B12-IF complex absorption in the terminal ileum | ~20-25% of seniors over 60 on metformin have B12 deficiency | 500-1,000mcg methylcobalamin sublingual daily; monitor B12 every 6 months |
| PPIs (omeprazole/Prilosec, pantoprazole/Protonix, esomeprazole/Nexium, lansoprazole/Prevacid) | Reduces gastric acid — impairs protein-bound B12 release from food; less relevant for free crystalline B12 in supplements | ~15% of seniors over 60 take PPIs long-term | 500-1,000mcg methylcobalamin (sublingual preferred — bypasses acid dependence) |
| H2 blockers (ranitidine/Zantac, famotidine/Pepcid) | Similar to PPIs but less potent acid reduction — milder B12 absorption impairment | Widely used OTC in seniors | 250-500mcg methylcobalamin if taking H2 blockers regularly |
| Antibiotics (chloramphenicol, neomycin long-term) | Disrupts gut bacteria involved in B12 metabolism; chloramphenicol specifically impairs B12 utilisation | Treatment-course exposure | Supplement during and 4 weeks after treatment course |
| Colchicine (gout medication) | Reduces ileal absorption of B12-IF complex | ~3-5% of seniors with gout | 250-500mcg methylcobalamin daily |
For a broader look at how digestive changes after 60 affect nutrient absorption including B12 beyond medication effects: Digestive Enzymes for Seniors — Why HCl Decline Causes B12 and Nutrient Malabsorption
Seniors managing blood sugar with metformin may also benefit from reviewing the berberine evidence — a botanical compound with comparable glucose-lowering mechanisms that does not carry the B12-depletion side effect. For the full clinical comparison: Berberine for Seniors — Blood Sugar, Cholesterol and Weight
Why 1,000mcg Is Not “Overdosing” — It’s Basic Math
The confusion about high-dose B12 disappears once you understand one number: 1%.
At doses above 500mcg, passive diffusion becomes the primary absorption route — and passive diffusion absorbs approximately 1% of the dose regardless of intrinsic factor status.
| Dose | Passively Absorbed | Reaches bloodstream |
|---|---|---|
| 100mcg | ~1mcg | Below deficiency threshold for most seniors |
| 500mcg | ~5mcg | Borderline for seniors with significant atrophic gastritis |
| 1,000mcg | ~10mcg | Meets minimum adequate intake for most seniors |
| 2,000mcg | ~20mcg | Target range for confirmed deficiency or neurological symptoms |
This is why your multivitamin’s 25mcg B12 does nothing for a senior with gastritis — and why 1,000mcg is the correct minimum, not an excessive dose.
Low stomach acid affects more than B12 — it is also the root cause of poor protein digestion, mineral malabsorption, and the bloating and indigestion that many seniors attribute to “getting older.” For the full explanation of how declining digestive enzyme production affects nutrient absorption after 60: Digestive Enzymes for Seniors — When Food Isn’t Enough
Top Vitamin B12 Products for Seniors — 2026 US Pricing
1. Jarrow Methyl B-12 1,000mcg Sublingual — Amazon — Best Overall
The most widely used senior B12 supplement on the market. Cherry-flavoured methylcobalamin sublingual lozenge at 1,000mcg — the right form, right dose, right route. Dissolves in approximately 60-90 seconds under the tongue. Available at most health food stores and online. ~$0.12-0.15/day. Best for: all seniors over 60, especially those on PPIs or with any absorption concern.
2. Life Extension Bioactive B12 Sublingual — Amazon / iHerb — Best Premium Formula
Combines methylcobalamin and adenosylcobalamin in a sublingual tablet — providing both active B12 coenzyme forms simultaneously for comprehensive B12 repletion covering both methylation cycle and mitochondrial energy functions. 1,000mcg total B12 per tablet. ~$0.20-0.28/day. Best for: seniors wanting complete B12 coenzyme coverage or those with significant fatigue alongside neurological symptoms.
3. Solgar Methylcobalamin 1,000mcg Sublingual — Amazon / Whole Foods — Best Allergen-Free
Methylcobalamin sublingual 1,000mcg. Free from gluten, wheat, dairy, soy, yeast, and artificial colours — the cleanest ingredient list available. NSF registered facility. ~$0.18-0.22/day. Best for: seniors with multiple food sensitivities or allergies, or those who prioritise minimal excipient formulations.
4. Garden of Life Vitamin B12 Spray — Amazon — Best for Swallowing Difficulties
Methylcobalamin oral spray — 500mcg per spray absorbed through oral mucosa. Particularly appropriate for seniors with dysphagia (swallowing difficulties) or those who struggle with tablet dissolution. ~$0.20-0.30/day at 1,000mcg dose (2 sprays). Best for: seniors with swallowing difficulties, those who find sublingual tablets difficult to hold in place.
5. NOW Foods Methyl B-12 1,000mcg Lozenges — Amazon / Walmart — Best Value
Methylcobalamin 1,000mcg lozenge at the lowest price point among quality methylcobalamin formulations. Available at Walmart for seniors who prefer in-store purchasing. ~$0.08-0.11/day. Best for: budget-conscious seniors who understand that methylcobalamin form is non-negotiable and want the best value available.
B12 Testing — When and What to Ask For
Routine annual bloodwork typically includes serum B12 only if specifically requested or if the physician includes a comprehensive metabolic panel with micronutrient assessment. Many seniors have never had their B12 tested despite being in the highest-risk age group. Proactive testing is warranted in these situations:
- Any senior over 65 — regardless of symptoms — should have serum B12 tested at least once to establish a baseline
- Any senior on metformin, PPIs, or H2 blockers for more than 12 months
- Any senior with fatigue, brain fog, memory changes, tingling or numbness in the extremities, or balance problems — these symptoms warrant B12 testing before other investigations
- Seniors following a vegetarian or vegan diet — no dietary B12 source exists in plant foods
- Seniors with a family history of pernicious anaemia — autoimmune destruction of parietal cells has a genetic component
When requesting testing, specify: serum B12 (routine, often included in comprehensive metabolic panels), methylmalonic acid (MMA) if serum B12 is in the borderline 200-400 pg/mL range (MMA elevation confirms functional deficiency even with borderline-normal serum B12), and total homocysteine if cardiovascular risk assessment is also relevant (B12 deficiency produces homocysteine elevation — a cardiovascular risk factor).
B12 and the Brain — The Neurological Stakes
Vitamin B12 is more critical to neurological health than any other B vitamin — and the neurological consequences of deficiency are the most clinically serious and the most time-sensitive reason to address senior B12 adequacy proactively.
Myelin Synthesis
Myelin — the fatty sheath that insulates nerve fibres and enables rapid signal transmission — requires methylcobalamin as a methyl donor for its synthesis. B12 deficiency causes demyelination — progressive loss of myelin from peripheral nerves and spinal cord tracts. Peripheral demyelination produces the tingling, numbness, and paraesthesia (pins and needles) in the hands and feet that are among the earliest neurological symptoms of deficiency. Spinal cord demyelination produces the subacute combined degeneration picture — weakness, balance problems, gait abnormalities, and in severe cases paralysis.
The clinical urgency: myelin synthesis requires continuous B12 availability. Once demyelination occurs, nerve regeneration is slow and incomplete — particularly in the spinal cord. The window for full neurological recovery narrows rapidly after the first 12 months of symptomatic deficiency, and spinal cord damage present for more than 24 months may not recover even with aggressive B12 repletion.
The Methylation Cycle and Cognitive Function
Methylcobalamin is essential for the methylation cycle — the biochemical pathway that converts homocysteine to methionine and then to S-adenosyl methionine (SAM-e). SAM-e is the universal methyl donor for over 200 methylation reactions in the body, including the synthesis of neurotransmitters (dopamine, serotonin, norepinephrine), the methylation of myelin proteins, and the regulation of gene expression through DNA methylation.
When B12 is deficient, the methylation cycle stalls: homocysteine accumulates (a vascular toxin associated with accelerated atherosclerosis and blood vessel damage), SAM-e production falls, and neurotransmitter synthesis declines. The cognitive consequence is the pattern familiar from the B12 deficiency symptom picture: brain fog, slowed thinking, word-finding difficulty, and memory impairment. This is chemically distinct from and additive with the cognitive impairments of vitamin D deficiency and magnesium insufficiency — and all three are common in seniors simultaneously.
B12 and Dementia Risk
Elevated homocysteine from B12 deficiency is an independent risk factor for dementia and Alzheimer’s disease in large population studies. The VITACOG trial found that B vitamin supplementation (including B12) significantly slowed brain atrophy on MRI in adults with mild cognitive impairment and elevated baseline homocysteine, with the greatest protection in those with the highest omega-3 levels — suggesting B12 and omega-3 work synergistically in brain preservation. While B12 supplementation has not been shown to reverse established dementia, maintaining adequate B12 throughout the 60s and 70s is among the most straightforward and evidence-supported dementia prevention strategies available.
Related Articles on SupplementsOver50.com
• Signs of Vitamin B12 Deficiency in Adults Over 60 — And What to Do
• 5 Best Multivitamins for Seniors — Which Ones Actually Provide Adequate B12?
• Best Multivitamin for Women Over 60 — B12 Form and Dose Matter
• Digestive Enzymes for Seniors — Why HCl Decline Causes Nutrient Malabsorption
• The 5 Essentials — Supplements Every Adult Over 60 Should Know
References
6. NIH Office of Dietary Supplements — Vitamin B12 Fact Sheet for Health Professionals (2024 update)
Frequently Asked Questions
Is 1,000mcg of B12 too much for seniors?
No — B12 has no established tolerable upper limit because it is water-soluble and excess is safely excreted in urine. The reason 1,000mcg is used is not that seniors need 400 times the RDA, but that passive diffusion absorbs approximately 1% of any oral dose. At 1,000mcg, passive diffusion delivers approximately 10mcg — well above the 2.4mcg RDA — through a pathway that works regardless of intrinsic factor status or stomach acid levels. There is no meaningful risk of overdose from oral methylcobalamin at 1,000-2,000mcg daily in adults with normal kidney function. If your physician recommends lower doses, the clinical concern is usually about other conditions elevating serum B12 artificially rather than toxicity from the supplement itself.
How do I know if my multivitamin provides enough B12?
Check three things on your multivitamin’s Supplement Facts panel. First, the form — if it says ‘cyanocobalamin’ rather than ‘methylcobalamin,’ the form is suboptimal and may be poorly utilised by the 30-40% of adults with MTHFR variants. Second, the dose — if it provides 6-25mcg, this is completely inadequate for any senior with absorption impairment, as passive diffusion of 25mcg delivers only 0.25mcg. Third, whether you have any absorption risk factors (age over 65, PPI use, metformin use, history of digestive issues) — if any apply, the multivitamin B12 dose is insufficient regardless of form. The solution: add a separate methylcobalamin sublingual supplement at 500-1,000mcg daily alongside your multivitamin rather than switching multivitamins.
What is the best time of day to take vitamin B12?
B12 can be taken at any time of day — it is water-soluble and does not require food for absorption. Morning is commonly recommended because B12 has mild energising properties through its role in red blood cell formation and neurological function — some seniors find evening doses cause mild sleep disruption, though this is uncommon. For sublingual forms, take on an empty stomach or at least away from a meal, hold under the tongue for 60-90 seconds before swallowing, and avoid eating or drinking for 5-10 minutes after to maximise mucosal absorption. Consistency of daily use at any time matters far more than precise timing.
How long does it take for B12 supplements to work?
Timeline varies significantly by symptom. Energy and fatigue: typically the first improvement noticed — often within 2-4 weeks of corrective supplementation at 1,000mcg daily as red blood cell production normalises and oxygen delivery to tissues improves. Brain fog and cognitive clarity: 4-8 weeks in most seniors with mild to moderate deficiency. Mood stabilisation: 4-12 weeks. Peripheral tingling and numbness: highly variable — mild cases may improve significantly within 4-8 weeks; moderate cases may take 3-6 months; severe cases may show only partial improvement and require physician management. The general principle: symptoms that developed over months typically resolve over weeks to months; symptoms that developed over years may take months to years and may not fully reverse, particularly neurological damage.
Can vitamin B12 deficiency cause permanent damage in seniors?
Yes — this is the most important urgency point about senior B12 deficiency. Neurological damage from B12 deficiency — specifically subacute combined degeneration of the spinal cord — can become permanent if not treated within approximately 12 months of onset. The spinal cord damage involves demyelination of the posterior and lateral columns, producing the classic picture of weakness, balance problems, and gait abnormalities. Peripheral nerve demyelination (tingling, numbness) is more reversible than spinal cord damage. Cognitive impairment from prolonged deficiency has variable recovery — early deficiency typically fully reverses; deficiency present for more than 2-3 years may produce residual cognitive changes. This is the reason not to delay physician assessment when neurological symptoms are present, rather than attempting to address them with oral supplementation alone.
Do seniors need B12 injections or will oral supplementation work?
For the majority of seniors with mild to moderate deficiency from age-related absorption decline or medication depletion, high-dose oral methylcobalamin at 1,000-2,000mcg daily (especially sublingual) is effective — the passive diffusion and mucosal absorption pathways work regardless of intrinsic factor status and deliver adequate B12 over 2-4 months. Intramuscular injections are indicated when: deficiency is severe (serum B12 below 150 pg/mL), neurological symptoms are already present and require rapid correction, complete pernicious anaemia with zero intrinsic factor production is confirmed, or oral supplementation has been tried at adequate doses for 3 months without improvement in blood levels. Injections typically use hydroxocobalamin IM — usually a loading schedule of weekly injections for 3 months followed by monthly maintenance. Many seniors prefer the convenience of daily oral sublingual supplementation over periodic injections once deficiency has been corrected to an adequate baseline.
Why do I need 1,000mcg of B12 if the RDA is only 2.4mcg?
The RDA of 2.4mcg assumes normal stomach acid and intrinsic factor production — the two-step active absorption pathway that works efficiently in healthy young adults. Most seniors over 60 have some degree of atrophic gastritis, which impairs both stomach acid production and intrinsic factor secretion, making the active pathway unreliable. At doses of 500mcg and above, a secondary passive diffusion pathway absorbs approximately 1% of the dose independently of intrinsic factor. So a 1,000mcg dose delivers roughly 10mcg through passive diffusion alone — just enough to maintain adequate serum levels in a senior with compromised active absorption. The high dose is not pharmacological excess; it is the mathematically correct compensation for a failing absorption system.
Can Metformin cause B12 deficiency?
Yes — and this is one of the most underdiagnosed medication-nutrient interactions affecting seniors. Metformin blocks the calcium-dependent transporters in the terminal ileum that are required for the intrinsic factor-B12 complex to bind and be absorbed. Approximately 20–30% of long-term metformin users develop clinically meaningful B12 deficiency, and the risk increases with dose and duration of use. Symptoms — fatigue, peripheral tingling, cognitive slowing — are often attributed to aging or diabetes itself rather than B12 depletion. Seniors on metformin should have serum B12 checked annually; if levels fall below 300 pg/mL, a high-dose sublingual methylcobalamin supplement at 1,000mcg daily is the standard correction approach.
Are sublingual B12 tablets better than regular swallowed B12?
For seniors with atrophic gastritis, low stomach acid, or those taking PPIs or H2 blockers, sublingual B12 is generally the better choice. Sublingual tablets dissolve under the tongue and allow B12 to be partially absorbed directly through the oral mucosa, bypassing the stomach acid and intrinsic factor steps entirely. This is not as efficient as healthy active absorption, but it reliably delivers meaningful B12 without depending on a digestive system that may be significantly impaired. For seniors with confirmed absorption problems — those on PPIs, metformin, or with known atrophic gastritis — sublingual methylcobalamin 1,000mcg is the recommended default over standard swallowed tablets.
The Bottom Line
The vitamin B12 dosing question for seniors has a clear and evidence-based answer: 500-1,000mcg methylcobalamin daily as a sublingual tablet for any senior with known or suspected absorption impairment; 25-100mcg methylcobalamin daily as a minimum maintenance dose for all seniors over 60 regardless of apparent health status. Always methylcobalamin — never cyanocobalamin. For malabsorbers, always sublingual — never swallowed tablets as the only B12 source.
The RDA of 2.4mcg is a number designed for young healthy adults with intact absorption — it is the minimum to prevent deficiency in someone who absorbs well, not a target for seniors whose absorption system has partially failed. The passive diffusion calculation — 1% of 1,000mcg = 10mcg absorbed regardless of intrinsic factor status — is the pharmacological logic that makes high-dose oral supplementation effective for the 30-40% of seniors with impaired active absorption.
Test your B12 if you have not done so recently. If your result is below 400 pg/mL and you are over 60, add sublingual methylcobalamin 1,000mcg daily to your protocol immediately. If you have any neurological symptoms — tingling, numbness, balance problems — see your physician before relying on oral supplementation alone.
For the full deficiency symptom guide including how to distinguish B12 from vitamin D and magnesium deficiency: Signs of Vitamin B12 Deficiency in Adults Over 60 — And What to Do
For the complete senior supplement foundation: The 5 Essentials — Supplements Every Adult Over 60 Should Know