| ⚕️ Medical Disclosure The symptoms described in this article including Signs of Magnesium Deficiency after 60 overlap with many other medical conditions. Do not self-diagnose magnesium deficiency or modify prescription medications based on symptoms alone. Standard serum magnesium blood tests miss deficiency in approximately 80% of affected adults — a normal result does not rule out deficiency. If you recognise multiple symptoms described here, discuss them with your physician and consider a supervised supplementation trial. This article does not constitute medical advice. |
| ⚡ Quick Answer Approximately 48% of US adults are magnesium deficient or insufficient — rising to an estimated 60-70% in adults over 60. The most common symptoms are muscle cramps and twitching, disrupted sleep, heart palpitations, anxiety and restlessness, persistent fatigue, and constipation. The critical limitation of standard blood tests: serum magnesium measures only 1% of total body magnesium. The body sacrifices bone and muscle stores to maintain blood levels within a narrow range — meaning serum magnesium appears normal until deficiency is severe. This is why the majority of deficient seniors are told their ‘labs are normal’ while experiencing multiple classic deficiency symptoms simultaneously. |
Why Magnesium Deficiency Is the Most Missed Nutritional Problem After 60
Magnesium participates in over 300 enzymatic reactions — energy production, DNA synthesis and repair, protein construction, nerve signal transmission, muscle contraction and relaxation, blood glucose regulation, and blood pressure control. The breadth of this involvement explains why deficiency produces such a diffuse and non-specific symptom picture. When ten different body systems are simultaneously underperforming because a single mineral is insufficient, the symptoms look less like a nutritional deficiency and more like the general deterioration of aging.
This is the central challenge with magnesium deficiency in seniors. Its symptoms are real and clinically significant — but they map so closely onto the expected experience of getting older that the majority of affected adults and their physicians never consider magnesium as the common thread. Fatigue, poor sleep, anxiety, muscle cramps, palpitations, constipation, headaches — each is common in older adults for dozens of reasons. When all six appear together, the most parsimonious explanation is often magnesium deficiency. Yet most clinical encounters address each symptom separately.
Recognising the symptom pattern is the first step — the next is knowing exactly how much to take and which form to choose for your specific situation: How Much Magnesium Should Seniors Take Daily? — Dosing by Form, Goal and Health Condition.
Three Reasons Deficiency Is So Common After 60
The biology of aging creates a perfect storm for magnesium insufficiency that does not exist at younger ages:
- Intestinal absorption efficiency declines — the TRPM6 and TRPM7 transporter channels that actively move magnesium across the gut wall decrease in expression with age, reducing absorption by approximately 20-30% per gram consumed versus young adulthood
- Renal reabsorption decreases — aging kidneys excrete more magnesium in urine per day, increasing daily losses and raising the effective dietary requirement
- Medication depletion becomes near-universal — PPIs (taken by approximately 15% of seniors) directly impair intestinal magnesium absorption; loop and thiazide diuretics (taken by approximately 25% of seniors) dramatically increase urinary magnesium excretion; these two medication classes alone mean that over one-third of all seniors over 60 have medically-induced magnesium depletion on top of age-related losses
The compounding effect: a 70-year-old woman taking omeprazole for GERD and hydrochlorothiazide for blood pressure has three simultaneous forces depleting her magnesium — age-related absorption decline, PPI-induced absorption impairment, and diuretic-induced excretion increase. Her effective magnesium requirement may be 150-200mg per day higher than the RDA to achieve the same tissue saturation as an unmedicated 30-year-old eating the same diet.
Popular Supplement Guides:

")




For the complete dosing guide including medication-adjusted targets: How Much Magnesium Should Seniors Take Daily? — Dosing by Form, Goal and Health Condition
Key Statistics
- 48% of US adults fail to meet the magnesium RDA — rising to an estimated 60-70% of adults over 60
- Average US dietary magnesium intake in adults over 60 is approximately 250mg for women and 320mg for men — below the respective RDAs of 320mg and 420mg
- Standard serum magnesium tests miss deficiency in approximately 80% of affected adults because only 1% of total body magnesium circulates in blood
- Magnesium deficiency is associated with a 2-fold higher risk of cardiovascular disease, 2.1-fold higher risk of diabetes, and significantly higher rates of depression in large population studies
- A 2022 review in Nutrients confirmed that magnesium deficiency is independently associated with accelerated telomere shortening — a direct marker of biological aging rate
- PPIs are associated with a 43% higher rate of clinically significant hypomagnesaemia in seniors versus non-users in large observational studies
The 10 Signs of Magnesium Deficiency After 60
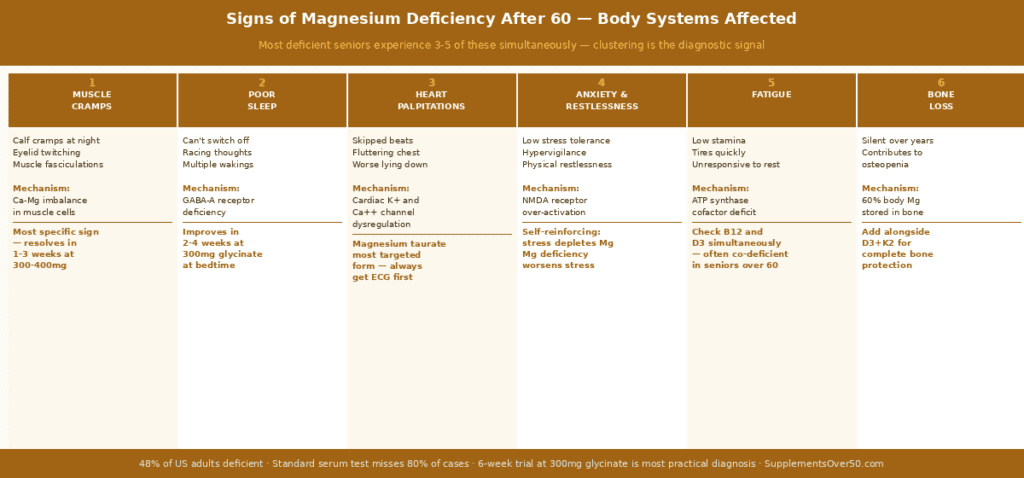
These symptoms are presented in order of clinical specificity — how strongly each one points toward magnesium deficiency versus other causes. The more symptoms from this list you recognise, and the more they cluster across multiple body systems simultaneously, the more likely magnesium deficiency is a significant contributing factor.
Sign 1 — Nighttime Muscle Cramps and Twitching
Involuntary muscle cramping — particularly in the calves, feet, and arches during sleep or immediately on waking — is the most recognisable and most specific sign of magnesium deficiency in older adults. Understanding why requires understanding the calcium-magnesium balance in muscle physiology.
Muscle contraction is triggered by calcium ions flooding into the muscle cell. Relaxation requires calcium to be actively pumped back out — a process that depends on magnesium-dependent calcium ATPase enzymes. When magnesium is insufficient, this calcium clearance pump underperforms: calcium lingers inside the muscle cell, the contraction signal is not terminated cleanly, and the muscle remains partially contracted or contracts involuntarily. The result is the sustained, painful cramping that wakes seniors from sleep.
Eyelid twitching (the flickering sensation under the eyelid that comes and goes), facial muscle fasciculations (small rippling movements visible under the skin), and general muscle restlessness in the legs — described as the sensation of needing to move the legs constantly, sometimes confused with restless leg syndrome — all share this calcium-magnesium mechanism.
The clinical distinguishing feature: magnesium-driven cramps typically resolve within 1-3 weeks of corrective supplementation at 300-400mg magnesium glycinate daily. If cramps resolve with supplementation, deficiency was likely the primary driver. If they persist despite adequate supplementation, other causes (electrolyte imbalance, circulation, neurological) warrant investigation.
Sign 2 — Poor Sleep — Difficulty Falling and Staying Asleep
Magnesium is one of the most physiologically important regulators of sleep architecture. It supports sleep through two distinct mechanisms that act on different aspects of the sleep problem common in older adults.
The first mechanism is GABA-A receptor activation. GABA (gamma-aminobutyric acid) is the brain’s primary inhibitory neurotransmitter — the neurochemical signal that says ‘stop firing, slow down, rest.’ Magnesium enhances the binding of GABA to GABA-A receptors, amplifying the brain’s natural quieting signal. In deficient adults, this signal is weakened — producing the hyperarousal state at bedtime that many seniors describe as an inability to ‘switch off’ despite feeling physically tired. The brain remains in a state of persistent low-level excitatory activity that prevents the transition to sleep.
The second mechanism is cortisol regulation. Magnesium modulates HPA axis activity and reduces the evening cortisol spike that, when elevated, directly suppresses melatonin production and delays sleep onset. Many seniors with magnesium deficiency experience a pattern of feeling alert and wired in the evening despite low daytime energy — this is the cortisol-magnesium connection: daytime fatigue from impaired ATP production combined with evening hyperarousal from inadequate cortisol buffering.
The characteristic magnesium sleep problem is distinct from other sleep disorders: difficulty initiating sleep rather than breathing-related waking (sleep apnea), middle-of-night waking with inability to return to sleep (common in anxiety and depression), or excessive sleepiness regardless of sleep duration (narcolepsy, thyroid). Magnesium deficiency specifically produces the pattern of lying awake at night despite fatigue, often with physical restlessness.
For the complete comparison of magnesium forms specifically for sleep, and the melatonin combination protocol: Best Magnesium for Sleep After 50 — Glycinate vs L-Threonate Explained
Sign 3 — Heart Palpitations and Cardiac Awareness
Awareness of the heartbeat — whether as palpitations, skipped beats, fluttering sensations, or racing episodes — is one of the more alarming symptoms of magnesium deficiency and one that consistently prompts seniors to seek medical attention. Cardiac evaluation is appropriate and important whenever palpitations occur. However, after structural and electrical causes have been excluded by ECG and appropriate workup, magnesium deficiency is one of the most common correctable causes of benign palpitations in adults over 60.
The mechanism involves magnesium’s role as a natural calcium channel regulator in cardiac cells. The electrical cycle of each heartbeat — depolarisation (calcium floods in, triggering contraction) followed by repolarisation (calcium exits, the cell resets) — depends on magnesium-dependent pumps and channels to execute precisely. When magnesium is deficient, the repolarisation process becomes irregular: calcium lingers in cardiac cells between beats, producing the ectopic beats and irregular firing that registers as palpitations.
Magnesium also regulates potassium channel function in the heart — and because potassium balance is interdependent with magnesium, deficiency in one frequently accompanies deficiency in the other. Seniors with low potassium (hypokalemia) who are not responding to potassium supplementation often have underlying magnesium deficiency preventing potassium repletion. Correcting magnesium first, then potassium, resolves the situation where correcting potassium alone failed.
The most cardiovascular-targeted magnesium form for this application is magnesium taurate — taurine adds independent antiarrhythmic properties including stabilisation of cardiac membrane potential and reduction of oxidative stress on the myocardium.
For the complete cardiovascular evidence — magnesium and blood pressure, AFib, and the taurate vs glycinate comparison: Magnesium for Heart Health and Blood Pressure After 50 — Full Evidence Guide
Sign 4 — Anxiety, Restlessness, and Low Stress Tolerance
Anxiety driven by magnesium deficiency has a characteristic quality that distinguishes it from primary anxiety disorders: it is predominantly physical rather than cognitive. Seniors with magnesium deficiency anxiety describe physical restlessness — an inability to physically relax, a constant low-level tension in the muscles, a sense of being ‘on edge’ without necessarily having worried thoughts — rather than the ruminative cognitive anxiety of generalised anxiety disorder.
The neurobiological mechanism involves two pathways. First, NMDA (N-methyl-D-aspartate) glutamate receptors — the primary excitatory receptors in the brain — are normally regulated by magnesium ions that physically block the channel at resting membrane potential. When magnesium is insufficient, this blockade weakens and NMDA receptors become hyperactive, producing excitotoxic-adjacent neuronal firing that manifests as anxiety, hypervigilance, and an exaggerated startle response.
Second, magnesium modulates HPA axis activity — reducing ACTH release from the pituitary and cortisol release from the adrenal glands. Deficiency removes this natural buffer on the stress response, allowing cortisol to rise more easily and remain elevated longer in response to ordinary daily stressors. Seniors with magnesium deficiency frequently describe a reduced capacity to handle stress that previously felt manageable — minor frustrations or inconveniences triggering a disproportionate physiological stress response.
The relationship between stress and magnesium deficiency is bidirectional and self-reinforcing: deficiency lowers stress tolerance, and chronic stress increases urinary magnesium excretion — creating a cycle that can produce escalating anxiety over months without a clear external trigger. This pattern is particularly common in seniors undergoing major life transitions including retirement, bereavement, or health challenges.
Sign 5 — Persistent Fatigue and Low Stamina
Magnesium is a required cofactor for ATP synthase — the enzyme that produces adenosine triphosphate (ATP) by harnessing the proton gradient built by the mitochondrial electron transport chain. Without adequate magnesium, this final step of cellular energy production is impaired: the physical structure of ATP requires magnesium (ATP exists primarily as the Mg-ATP complex in cells), and ATP synthase requires magnesium for its catalytic function.
The fatigue of magnesium deficiency is therefore not hunger-driven or sleep-driven — it is a fundamental impairment of cellular energy chemistry. Seniors describe it as a reduction in stamina rather than a reduction in energy at rest: the capacity to begin tasks remains largely intact but sustaining them is disproportionately tiring. Carrying groceries, climbing stairs, walking longer distances, and sustained mental concentration all require more effort than expected and produce more fatigue than the activity level should justify.
This fatigue pattern has significant overlap with vitamin D deficiency fatigue — both impair cellular energy production through different mechanisms, and both are extremely common in seniors. When fatigue is the primary complaint in an adult over 60, the most efficient clinical approach is to address both magnesium and vitamin D simultaneously rather than one at a time, since co-deficiency is statistically likely and both are safe to supplement concurrently. The D3 activation co-dependency means that seniors with both deficiencies frequently see their vitamin D blood levels fail to respond to supplementation until magnesium is also corrected — a pattern that explains many puzzling cases of persistent D3 deficiency despite supplementation: Signs of Vitamin D Deficiency in Seniors — 11 Symptoms Most Adults Miss After 60.
For the full vitamin D deficiency picture including the fatigue overlap and testing guide: Signs of Vitamin D Deficiency in Seniors — 11 Symptoms Most Adults Miss After 60
Sign 6 — Constipation and Slowed Gut Motility
Magnesium supports intestinal motility through its role as a calcium antagonist in intestinal smooth muscle. The peristaltic contractions that move food through the digestive tract require smooth muscle to contract and then relax rhythmically. Magnesium enables the relaxation phase — without it, intestinal smooth muscle tends toward tonic contraction rather than rhythmic peristalsis, slowing transit time and contributing to constipation.
This mechanism works in the same direction as the muscle cramp mechanism — inadequate magnesium impairs the calcium clearance that enables muscle relaxation, whether in skeletal muscle (producing cramps), cardiac muscle (producing palpitations), or smooth muscle in the gut wall (producing constipation and slowed motility). Seniors experiencing both muscle cramps and constipation simultaneously have a particularly clear clinical picture pointing toward magnesium insufficiency.
Note the distinction between magnesium’s intrinsic motility-supporting role (present with absorbed forms at appropriate doses) and the pharmacological laxative effect of high-dose magnesium oxide or citrate (which works by drawing water into the colon osmotically — a completely different and unrelated mechanism). Correcting magnesium deficiency with glycinate or malate supports normal gut motility without the unpredictable laxative effect.
Sign 7 — Headaches and Increased Migraine Frequency
Magnesium deficiency is among the most well-established non-pharmaceutical risk factors for both tension headaches and migraine in adults. The American Headache Society and the American Academy of Neurology both recognise magnesium deficiency as a significant contributing factor to migraine pathophysiology — and magnesium supplementation is included in migraine prevention guidelines as a level B recommendation (probable effectiveness). Once you have identified the symptom pattern, choosing the right form is critical — magnesium oxide found in most cheap supplements absorbs at only 4% and will not correct deficiency regardless of the dose on the label: 5 Best Magnesium Supplements for Seniors — Ranked by Form and Use Case.
The mechanisms are multiple: magnesium regulates cerebral blood vessel tone (deficiency allows vasospasm), modulates serotonin receptors involved in migraine pathophysiology, reduces cortical spreading depression (the electrical wave associated with migraine aura), and inhibits platelet aggregation that contributes to the vascular component of migraine. In adults with migraine, serum and cerebrospinal fluid magnesium levels are significantly lower during attacks than between episodes — suggesting that a magnesium-depleted state is not just associated with but mechanistically involved in migraine generation.
For seniors experiencing increased headache frequency — particularly if migraines have become more frequent in recent years without a clear precipitating factor — magnesium deficiency is worth excluding before escalating to pharmacological prophylaxis. The evidence base supports 400mg magnesium glycinate or citrate daily as migraine prevention, with trials showing 20-40% reduction in attack frequency in deficient adults.
Sign 8 — Bone Loss and Osteopenia Progression
Bone health is typically discussed in terms of calcium, vitamin D, and K2. Magnesium is frequently omitted from this conversation despite being a critical structural and regulatory component of bone physiology. Approximately 60% of total body magnesium is stored in bone matrix — it is structurally incorporated into the hydroxyapatite crystal lattice that gives bone its mineral density, and it influences the crystal size and stability that determine bone strength.
Beyond its structural role, magnesium regulates parathyroid hormone (PTH) secretion. PTH is the hormone that mobilises calcium from bone when blood calcium drops — elevated PTH (hyperparathyroidism, or even subclinical elevations from inadequate calcium absorption) accelerates bone breakdown. Magnesium deficiency impairs PTH regulation, producing a state of functional PTH resistance that further disrupts calcium homeostasis and bone metabolism.
Magnesium deficiency also impairs the vitamin D activation that is essential for calcium absorption. A senior with simultaneous magnesium and vitamin D deficiency — an extremely common combination — has impaired calcium absorption from both insufficiencies simultaneously, with calcium being drawn from bone to maintain blood levels despite supplementation.
The practical consequence: seniors taking calcium supplements and vitamin D3 for bone health but not magnesium may be experiencing suboptimal outcomes from their bone health protocol simply because the magnesium cofactor for D3 activation is missing. This is why the complete bone density protocol includes magnesium alongside D3, K2, and collagen.
Sign 9 — High Blood Pressure — The Silent Cardiovascular Connection
Magnesium functions as a natural calcium channel blocker in vascular smooth muscle. Calcium ions in arterial smooth muscle cells trigger vasoconstriction — narrowing of blood vessels and increased resistance that raises blood pressure. Magnesium counteracts this by competing with calcium at the same channel sites, promoting arterial dilation and reduced vascular resistance.
A 2025 meta-analysis of 38 clinical trials confirmed that magnesium supplementation reduces systolic blood pressure by an average of 2.81 mmHg and diastolic by 2.0 mmHg. While these average reductions appear modest, they are meaningful for two reasons. First, they are averaged across all participants — including many with normal blood pressure who show minimal change. Seniors with elevated baseline blood pressure and confirmed magnesium deficiency show substantially larger reductions. Second, even modest population-level blood pressure reductions translate to significant reductions in cardiovascular event rates — a 2 mmHg average systolic reduction is associated with approximately 7% lower stroke risk at the population level.
For seniors with borderline hypertension (systolic 120-139 mmHg) who want to avoid or delay medication, magnesium correction is among the most evidence-supported non-pharmaceutical interventions alongside dietary sodium reduction and exercise.
Sign 10 — Cognitive Decline, Poor Concentration, and Memory Difficulties
Magnesium’s role in cognitive function operates through several converging mechanisms. In the hippocampus — the brain region most critical for new memory formation — magnesium regulates synaptic plasticity through its control of NMDA receptor activity. NMDA receptors are required for long-term potentiation (LTP) — the process by which repeated activation of neural pathways strengthens their connections, the cellular correlate of learning and memory. Adequate magnesium is required for proper NMDA receptor regulation; too little impairs LTP and weakens memory consolidation.
Magnesium L-threonate — the blood-brain barrier-crossing form — has been shown to specifically increase hippocampal synaptic density, suggesting that magnesium deficiency may contribute to the synaptic pruning observed in age-related cognitive decline. A 2016 RCT found significant improvements in executive function and working memory in adults 50-70 taking magnesium L-threonate at 1.5-2g daily compared to placebo.
Beyond the hippocampal mechanism, the cellular energy impairment of magnesium deficiency directly affects cognitive function — the brain is the most energy-intensive organ per gram of tissue, and any impairment of ATP production preferentially affects the sustained mental effort required for concentration, complex problem-solving, and working memory tasks.
The cognitive symptoms of magnesium deficiency are often described as brain fog rather than memory loss — difficulty maintaining focus, slowing of mental processing, reduced capacity for sustained concentration — rather than the episodic memory failures more characteristic of B12 deficiency or early dementia. When brain fog is the primary cognitive complaint in an adult over 60, assessing and correcting magnesium (and vitamin D and B12) before pursuing neurological investigation is clinically appropriate.
The Symptom Clustering Pattern — Why Multiple Signs Together Matter
Individual magnesium deficiency symptoms are non-specific — every symptom on the list above has multiple other possible causes. The diagnostic power comes from clustering: multiple symptoms from different body systems appearing simultaneously in the same person is significantly more likely to indicate a single systemic nutritional cause than to represent coincidental independent diseases in each system.
| Symptom cluster | Body systems affected | Probability of Mg as driver | Recommended action |
| Muscle cramps + poor sleep + fatigue | Muscular, neurological, mitochondrial | High — classic triad | Serum Mg and 6-week glycinate trial at 300mg daily |
| Palpitations + anxiety + poor sleep | Cardiac, neurological, cortisol | High — HPA-cardiac cluster | Serum Mg; consider Mg taurate 300-400mg; ECG to exclude cardiac cause |
| Constipation + muscle cramps + fatigue | Gut, muscular, mitochondrial | High — smooth + skeletal muscle pattern | Mg glycinate 300mg — addresses all three through same Ca mechanism |
| Headaches + anxiety + poor sleep | Neurological across three domains | Moderate-high | Serum Mg; Mg glycinate or citrate 400mg daily; 4-6 week trial |
| Bone loss progression + fatigue + constipation | Skeletal, mitochondrial, gut | Moderate | Check Mg and D3 status; add Mg glycinate 300mg alongside D3+K2 protocol |
| Cognitive decline + fatigue + poor sleep | Neurological, mitochondrial, cortisol | Moderate — check B12 and D3 first | Confirm B12 and D3 adequate first; then consider Mg L-threonate 1.5-2g |
Why Standard Blood Tests Miss Magnesium Deficiency
This is the most clinically important and most underappreciated aspect of magnesium deficiency: standard serum magnesium testing is a poor diagnostic tool for the deficiency that affects the majority of seniors. Understanding why requires understanding magnesium distribution in the body.
Total body magnesium is distributed as follows: approximately 60% in bone matrix, 39% in muscle and soft tissues (primarily inside cells), and only 1% in extracellular fluid including blood plasma. The body treats blood magnesium levels as a narrow-range regulated variable — analogous to blood pH and blood glucose. When dietary magnesium intake drops or losses increase, the body draws from bone and muscle stores to maintain serum levels within the normal range (0.7-1.0 mmol/L).
This means serum magnesium remains normal throughout the entire period during which bone and muscle stores are being depleted — appearing reassuringly normal on a blood panel while the functional deficiency worsens. Serum magnesium only falls below the normal reference range when stores are severely depleted — at which point clinical hypomagnesaemia is severe and symptomatic.
The practical consequence: a senior with three months of muscle cramps, poor sleep, and palpitations whose serum magnesium comes back at 0.82 mmol/L (within the 0.7-1.0 normal range) is told their magnesium is fine — when they may have been drawing down bone and muscle stores for months to maintain that normal blood level.
More Accurate Assessment Methods
Three testing approaches provide more accurate information about functional magnesium status than serum magnesium:
- Red blood cell (RBC) magnesium: measures magnesium inside red blood cells rather than in plasma — reflects intracellular magnesium more accurately than serum. Requires a specific order from your physician and is not included in standard panels.
- 24-hour urinary magnesium excretion: measures how much magnesium the kidneys are excreting. Low urinary excretion alongside symptoms suggests the body is conserving magnesium due to depleted stores.
- Therapeutic trial: the most practical and accessible diagnostic approach. A 6-8 week trial of magnesium glycinate at 300mg daily is both diagnostic and therapeutic — symptom improvement confirms functional deficiency was contributing. No blood test required and the cost is minimal.
The therapeutic trial approach is particularly useful for primary care contexts where ordering RBC magnesium is uncommon. If three or more symptoms from the list above are present, a supervised supplementation trial is clinically reasonable and is increasingly recommended in functional medicine guidance for seniors.
Who Is at Highest Risk After 60
Certain subgroups of seniors over 60 face a substantially higher risk of clinically significant magnesium deficiency and should consider proactive supplementation even in the absence of overt symptoms:
| Risk factor | Mechanism | Estimated prevalence in seniors | Recommended action |
| On PPIs (omeprazole, pantoprazole, esomeprazole, lansoprazole) | Reduces intestinal Mg absorption — FDA 2011 warning | ~15% of seniors over 60 | Supplement at 300-400mg; serum Mg if on PPIs >1 year |
| On loop diuretics (furosemide/Lasix) | Directly increases urinary Mg excretion | ~10% of seniors over 60 | Supplement at 350-400mg; physician often orders periodic serum Mg |
| On thiazide diuretics (HCTZ, chlorthalidone) | Moderately increases urinary Mg excretion | ~18% of seniors over 60 | Supplement at 300-400mg daily |
| Type 2 diabetes | Magnesium deficiency worsens insulin resistance; metformin reduces absorption | ~25% of seniors over 60 | 300-400mg daily alongside B12 monitoring if on metformin |
| Alcohol use (even moderate chronic) | Alcohol dramatically increases urinary Mg excretion | Significant prevalence | 300-400mg daily; discuss alcohol intake with physician |
| Poor dietary variety / small appetite | Low dietary magnesium intake baseline | Common in over-70s especially | 300mg daily to compensate for dietary shortfall |
What to Do If You Recognise Multiple Symptoms
If you recognise three or more of the symptoms described in this article — particularly if they cluster across multiple body systems simultaneously — here is the practical action sequence:
- Step 1: Discuss with your physician. Describe the symptom cluster and request a serum magnesium test — not because a normal result rules out deficiency, but because it establishes a baseline and may identify frank hypomagnesaemia requiring more aggressive management.
- Step 2: Review your medication list. If you take a PPI, loop diuretic, thiazide diuretic, or metformin, you have medically-induced magnesium depletion on top of any age-related losses. Inform your physician that you want to address this.
- Step 3: Start magnesium glycinate 100-150mg daily with your evening meal. This is a safe starting dose for virtually all seniors with normal kidney function and establishes tolerability.
- Step 4: Increase gradually. Every two weeks, add 50mg to your daily dose until you reach 300mg. This gradual titration prevents the GI side effects (loose stools) that cause most seniors to abandon magnesium supplementation prematurely.
- Step 5: Evaluate at 6-8 weeks. Muscle cramps should have reduced significantly. Sleep quality should be noticeably better. Palpitations should be less frequent or absent. Anxiety and restlessness should have eased. If all these improvements occur, magnesium deficiency was almost certainly a significant contributing factor.
- Step 6: Maintain consistently. Unlike some supplements where effects plateau, magnesium’s benefits require ongoing daily supplementation — the deficiency will return if supplementation is discontinued while dietary intake remains below requirements.
For the complete dosing guide with form comparisons, medication adjustments, and product recommendations: How Much Magnesium Should Seniors Take Daily? — Dosing by Form, Goal and Health Condition
Magnesium and Vitamin D — The Co-Deficiency Most Seniors Have
One of the most clinically important patterns in senior nutrition is the simultaneous presence of magnesium and vitamin D deficiency in the same individual — an estimated 48% of US adults are magnesium insufficient and approximately 42% are vitamin D deficient, with substantial overlap between these populations.
The co-deficiency matters beyond simple addition of two nutritional gaps. Magnesium is a required cofactor for the enzymatic conversion of storage vitamin D (25-hydroxyvitamin D) to the active hormone form (1,25-dihydroxyvitamin D). Without adequate magnesium, this conversion step is impaired — meaning seniors can take vitamin D3 supplements for months and fail to see their blood levels reach the 40-60 ng/mL target range, not because their D3 dose is insufficient but because the magnesium co-factor is limiting the conversion.
This explains a frustrating clinical pattern: a senior is told their vitamin D is low, they start supplementing 2,000-4,000 IU D3 daily, but retesting at 3 months shows little improvement in blood levels. In many such cases, correcting magnesium deficiency simultaneously causes D3 blood levels to rise substantially without any change in the D3 dose. The magnesium was the rate-limiting factor.
For the vitamin D deficiency symptom picture and how to tell apart D3 deficiency from magnesium deficiency when symptoms overlap: Signs of Vitamin D Deficiency in Seniors — 11 Symptoms Most Adults Miss After 60
Related Articles on SupplementsOver50.com
• How Much Magnesium Should Seniors Take Daily? — Dosing by Form, Goal and Health Condition
• 5 Best Magnesium Supplements for Seniors — Ranked by Form and Use Case
• Best Magnesium for Sleep After 50 — Glycinate vs L-Threonate Explained
• Magnesium for Heart Health and Blood Pressure After 50 — Full Evidence Guide
• Signs of Vitamin D Deficiency in Seniors — 11 Symptoms Most Adults Miss After 60
• Signs of Vitamin B12 Deficiency in Adults Over 60 — And What to Do
• The 5 Essentials — Supplements Every Adult Over 60 Should Know
References
5. FDA 2011: Drug Safety Communication — Low magnesium levels associated with long-term PPI use
6. NIH Office of Dietary Supplements — Magnesium Fact Sheet for Health Professionals (2024 update)
Frequently Asked Questions
What are the first signs of magnesium deficiency in adults over 60?
The earliest and most consistent early signs are nighttime muscle cramps (particularly in the calves and feet), difficulty falling asleep despite feeling tired, and increased frequency of heart palpitations or cardiac awareness. These three symptoms often appear together in the early stages of deficiency — weeks to months before more obvious signs like pronounced fatigue, significant anxiety, or measurable changes in blood pressure. If you recognise any two of these three simultaneously, magnesium deficiency is a reasonable first consideration — particularly if you take a PPI, diuretic, or metformin that actively depletes magnesium.
Can magnesium deficiency cause heart palpitations in seniors?
Yes — benign palpitations are one of the most common and most alarming manifestations of magnesium deficiency in older adults. Magnesium regulates calcium channel function in cardiac cells; deficiency allows irregular calcium movement that produces ectopic beats, palpitation sensations, and occasional racing heart episodes. The characteristic pattern is palpitations most noticeable when lying down or at rest — the cardiac awareness that becomes prominent when physical distractions of daytime activity are removed. Always get palpitations evaluated by a physician to exclude structural and electrical causes. Once these are excluded, magnesium taurate at 300-400mg daily is the most cardiovascular-targeted supplementation approach.
How is magnesium deficiency diagnosed if blood tests are inaccurate?
The most practical diagnostic approach for most seniors is the therapeutic trial: 6-8 weeks of magnesium glycinate at 300mg daily, with structured symptom tracking at weeks 2, 4, and 8. Significant improvement in muscle cramps, sleep quality, or palpitations during this trial confirms that functional deficiency was contributing — without requiring specialist testing. For those who want laboratory confirmation, red blood cell (RBC) magnesium testing is more accurate than serum magnesium and reflects intracellular stores. Ask your physician to order ‘RBC magnesium’ specifically — standard metabolic panels and comprehensive blood panels typically include only serum magnesium.
Does magnesium deficiency cause anxiety in seniors?
Yes — physical anxiety driven by NMDA glutamate receptor hyperactivity and HPA axis dysregulation is a well-documented consequence of magnesium deficiency. The anxiety of deficiency is characteristically physical rather than cognitive: muscle tension, physical restlessness, exaggerated startle response, and difficulty physically relaxing — rather than ruminative worried thoughts. The bidirectional relationship between stress and magnesium (stress depletes magnesium; deficiency worsens stress response) creates a self-reinforcing cycle that can produce escalating anxiety over months without obvious external cause. Magnesium glycinate or L-threonate at 300-400mg daily typically produces significant anxiety reduction within 4-6 weeks in deficient adults.
Can fixing magnesium deficiency improve bone density?
Magnesium contributes to bone density through three mechanisms: structural incorporation into the hydroxyapatite crystal lattice (approximately 60% of body magnesium is stored in bone), regulation of PTH secretion that governs bone remodelling balance, and activation of vitamin D that enables calcium absorption. Correcting magnesium deficiency alongside vitamin D3 and K2 produces significantly better bone density outcomes than D3 and K2 alone — both because magnesium is directly needed in bone matrix and because D3 cannot be properly activated without it. A 2017 review in Osteoporosis International confirmed magnesium supplementation improves bone mineral density parameters in deficient adults.
Why do I feel worse after starting magnesium?
Loose stools or mild GI discomfort after starting magnesium supplementation almost always means the form is wrong or the dose is too high for your gut. Magnesium oxide and citrate pull water into the colon osmotically — this is uncomfortable and often misinterpreted as an adverse reaction when it is simply a form problem. Switch to magnesium glycinate and restart at 100mg daily with food. Glycinate is chelated to glycine and absorbs primarily through amino acid transporters rather than the osmotic mechanism — most seniors tolerate 300-400mg glycinate daily without any GI effects once the gradual titration is complete. If dizziness or unusual fatigue occurs after starting magnesium, check with your physician — this can occasionally indicate an interaction with blood pressure medications as magnesium’s vasodilatory effect adds to antihypertensive effects.
Why does my magnesium test show as normal if I have symptoms?
Standard serum magnesium only measures the 1% of total body magnesium circulating in your blood plasma. Your body treats blood magnesium as a tightly regulated variable — like blood pH — and will draw from bone and muscle stores to keep it within the normal range even as those stores are being significantly depleted. This means serum magnesium appears reassuringly normal throughout the entire period during which functional deficiency is developing and worsening. By the time serum magnesium actually falls below the reference range, cellular deficiency is typically severe and long-standing. A normal serum magnesium result does not rule out deficiency — it simply means your body has been successfully compensating at the expense of bone and muscle stores.
Can magnesium deficiency cause heart palpitations in seniors?
Yes — benign palpitations are one of the most consistent and clinically significant manifestations of magnesium deficiency in older adults. Magnesium is essential for maintaining cardiac electrical stability by regulating calcium channel function in myocardial cells. When magnesium is insufficient, the repolarisation phase between heartbeats becomes irregular — calcium lingers in cardiac cells after contraction, producing ectopic firing that registers as palpitations, skipped beats, or premature ventricular contractions (PVCs). The palpitations of magnesium deficiency are characteristically most noticeable when lying down at rest — when physical distractions are removed and cardiac awareness increases. Always have palpitations assessed by a physician to exclude structural causes. Once structural causes are excluded, magnesium taurate at 300-400mg daily is the most cardiovascular-targeted form for correction.
Is there a more accurate test than the standard serum magnesium blood test?
Yes — the red blood cell (RBC) magnesium test measures magnesium inside red blood cells rather than in plasma, reflecting intracellular magnesium status more accurately than serum. It must be specifically ordered as it is not included in standard metabolic panels. Ask your physician for “RBC magnesium” by name. Even RBC magnesium can miss deficiency in some contexts — 24-hour urinary magnesium excretion is another option, where low excretion alongside symptoms confirms the body is conserving magnesium due to depleted stores. The most accessible and practical diagnostic option for most seniors is a supervised therapeutic trial: 6-8 weeks of magnesium glycinate at 300mg daily with structured symptom tracking. Significant improvement during the trial confirms that functional deficiency was contributing — requiring no specialist testing.
Can magnesium deficiency cause anxiety in older adults?
Yes — and it is one of the most underappreciated connections in senior mental health. Magnesium deficiency produces physical anxiety through two distinct neurological mechanisms. First, NMDA glutamate receptors — the brain’s primary excitatory receptors — are normally gated by magnesium ions that block the channel at resting potential. When magnesium is insufficient, this blockade weakens and NMDA receptors become hyperactive, producing excitotoxic neuronal firing that manifests as physical restlessness, hypervigilance, and an exaggerated startle response. Second, magnesium modulates HPA axis activity — buffering cortisol release in response to stressors. Deficiency removes this buffer, allowing cortisol to rise more easily and persist longer. The result is a self-reinforcing cycle: deficiency worsens stress response, and chronic stress depletes magnesium further through increased urinary excretion.
How quickly does magnesium supplementation relieve muscle cramps?
Most seniors notice significant reduction in nighttime muscle cramp frequency and severity within 1-3 weeks of consistent supplementation at 300-400mg magnesium glycinate daily. The calcium-magnesium balance in muscle cells normalises relatively quickly once serum and tissue magnesium levels begin rising. Complete resolution of cramping — particularly in seniors who have been deficient for months or years — may take 4-6 weeks as bone and muscle stores gradually replenish. If cramps do not improve after 4 weeks at 300mg glycinate, consider increasing to 400mg before concluding that magnesium is not the driver. Persistent cramping despite adequate supplementation warrants assessment for other electrolyte imbalances, circulatory issues, or neurological causes.
Does magnesium deficiency affect bone density in seniors?
Yes — through three mechanisms that make magnesium as important to bone health as calcium and vitamin D, despite being far less discussed. First, approximately 60% of total body magnesium is structurally incorporated into bone mineral matrix — chronic deficiency directly reduces the mineral that bones are made of. Second, magnesium regulates parathyroid hormone (PTH) secretion, which governs the balance between bone formation and resorption — deficiency disrupts this balance toward net bone loss. Third, magnesium is the cofactor required for vitamin D activation — without adequate magnesium, supplemental D3 cannot be converted to its active hormone form and cannot support calcium absorption for bone mineralisation. Seniors supplementing D3 and K2 for bone health who are simultaneously magnesium deficient are getting significantly less bone protection from their bone health protocol than they would with magnesium included.
The Bottom Line
Magnesium deficiency is the most common unrecognised nutritional problem in adults over 60 — affecting an estimated 60-70% of this population to some degree while standard blood tests miss the majority of cases. The 10 symptoms described in this guide range from immediately obvious (nighttime muscle cramps, palpitations, disrupted sleep) to subtle and long-term (progressive bone loss, cognitive decline, escalating anxiety).
The diagnostic approach is pragmatic: recognise the symptom clustering pattern, consider medication-induced depletion if relevant to your situation, and conduct a structured 6-8 week therapeutic trial of magnesium glycinate 300mg daily. Symptom improvement is both diagnostic confirmation and therapeutic benefit simultaneously. No specialist referral required, minimal cost, and an excellent safety profile in seniors with normal kidney function.
The co-deficiency with vitamin D is particularly important — if your vitamin D supplementation has not been producing the expected blood level improvements, magnesium deficiency limiting D3 activation may be the reason. Correcting both simultaneously is more efficient than addressing either alone.
For the complete dosing guide and form comparisons: How Much Magnesium Should Seniors Take Daily? — Dosing by Form, Goal and Health Condition
For product recommendations at every price point: 5 Best Magnesium Supplements for Seniors — Ranked by Form and Use Case